

Clinical utilities of quantitative ultrasound in osteoporosis associated with inflammatory rheumatic diseases
- PMID: 29541626
- PMCID: PMC5835660
- DOI: 10.21037/qims.2018.02.02
Clinical utilities of quantitative ultrasound in osteoporosis associated with inflammatory rheumatic diseases
Abstract
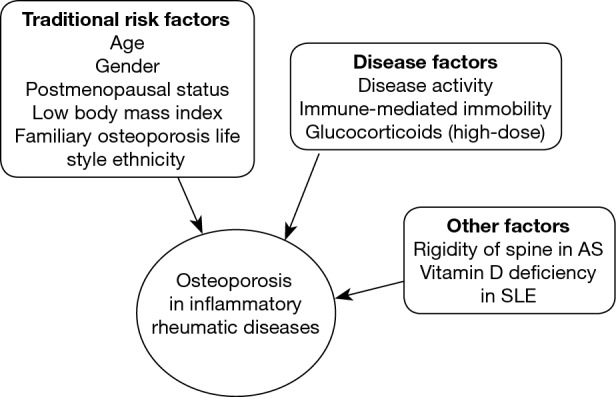
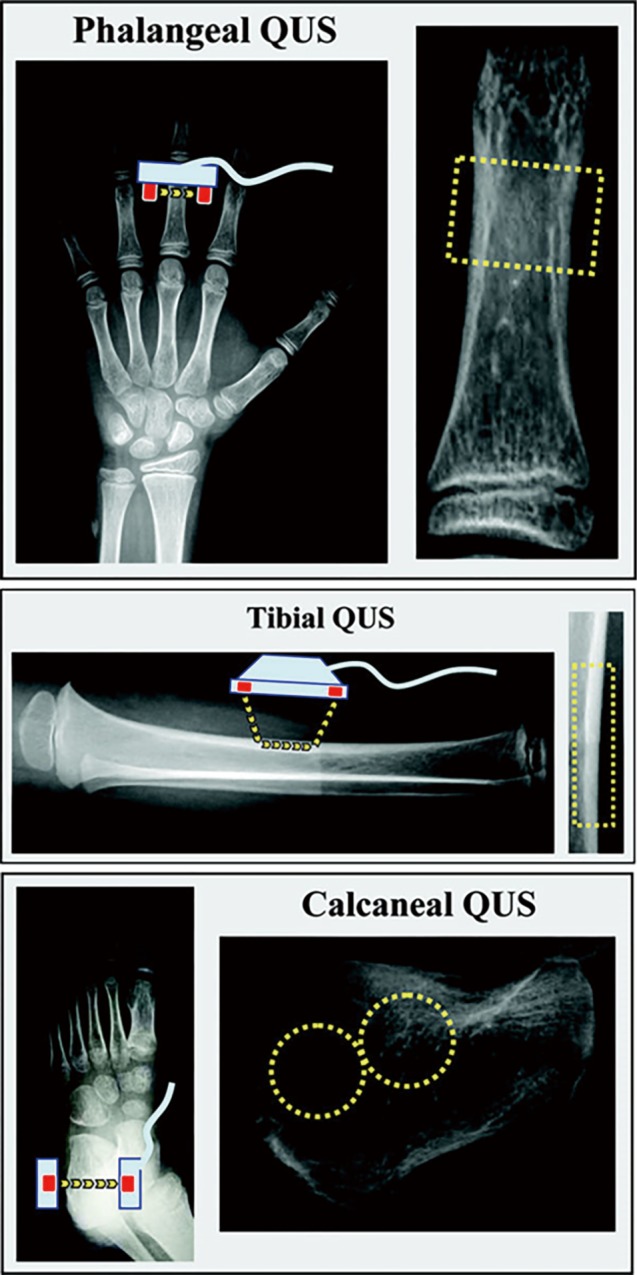
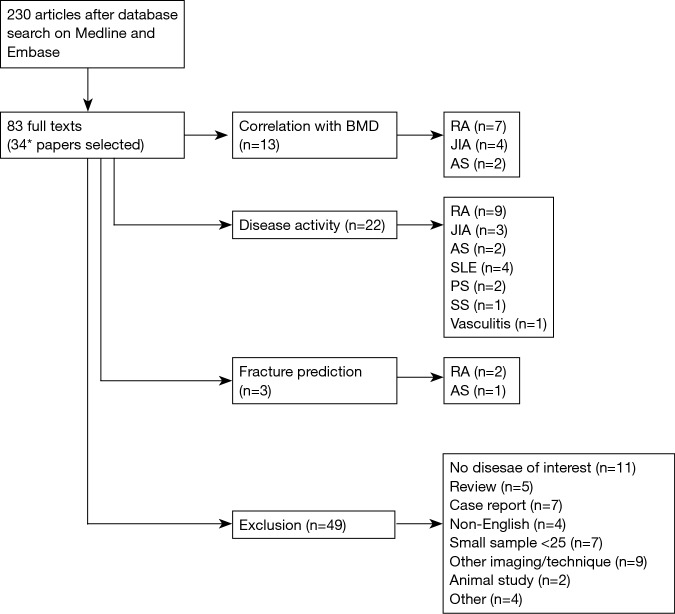
Secondary osteoporosis is an important co-morbidity related to inflammatory rheumatic diseases that is attributed to several factors including inflammatory cytokines, inactivity and glucocorticoid treatment. Quantitative ultrasound (QUS) has been utilized in osteoporosis research due to its detectability of bone density as well as bone quality. The current narrative review is to address the potential utilities of QUS in secondary osteoporosis of inflammatory rheumatic diseases, focusing on the clinical aspects of QUS in these diseases, based on the conformity of QUS with dual emission X-ray absorptiometry (DXA), the relationship with disease characteristics, and its capability of fracture prediction. Although limited data demonstrate that QUS had moderate to strong correlation with DXA, and might be useful as a potential imaging tool to screen for osteoporosis, further research is still required for QUS to be utilized effectively for the best outcome in these patients with rheumatic diseases.
Keywords: Quantitative ultrasound (QUS); fracture; inflammatory rheumatic disease; osteoporosis; review.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser 1994;843:1-129. - PubMed
-
- Gordon CM, Baim S, Bianchi ML, Bishop NJ, Hans DB, Kalkwarf H, Langman C, Leonard MB, Plotkin H, Rauch F, Zemel BS. Special report on the 2007 Pediatric Position Development Conference of the International Society for Clinical Densitometry. South Med J 2008;101:740-3. 10.1097/SMJ.0b013e31817a8b55 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources