

Association of Albuminuria With Major Adverse Outcomes in Adults With Congenital Heart Disease: Results From the Boston Adult Congenital Heart Biobank
- PMID: 29541749
- PMCID: PMC5875351
- DOI: 10.1001/jamacardio.2018.0125
Association of Albuminuria With Major Adverse Outcomes in Adults With Congenital Heart Disease: Results From the Boston Adult Congenital Heart Biobank
Abstract
Importance: Albuminuria is associated with adverse outcomes in diverse groups of patients, but the importance of albuminuria in the emerging population of increasingly complex adults with congenital heart disease (ACHD) remains unknown.
Objective: To assess the prevalence, risk factors, and prognostic implications of albuminuria in ACHD.
Design, setting, and participants: This prospective study assessed a cohort of ambulatory patients aged 18 years and older who were examined at an ACHD referral center and enrolled in the Boston ACHD Biobank between May 17, 2012, to August 5, 2016. Albuminuria was defined as an urine albumin-to-creatinine (ACR) ratio of 30 mg/g or more.
Main outcomes and measures: Death or nonelective cardiovascular hospitalization, defined as overnight admission for heart failure, arrhythmia, thromboembolic events, cerebral hemorrhage, and/or disease-specific events.
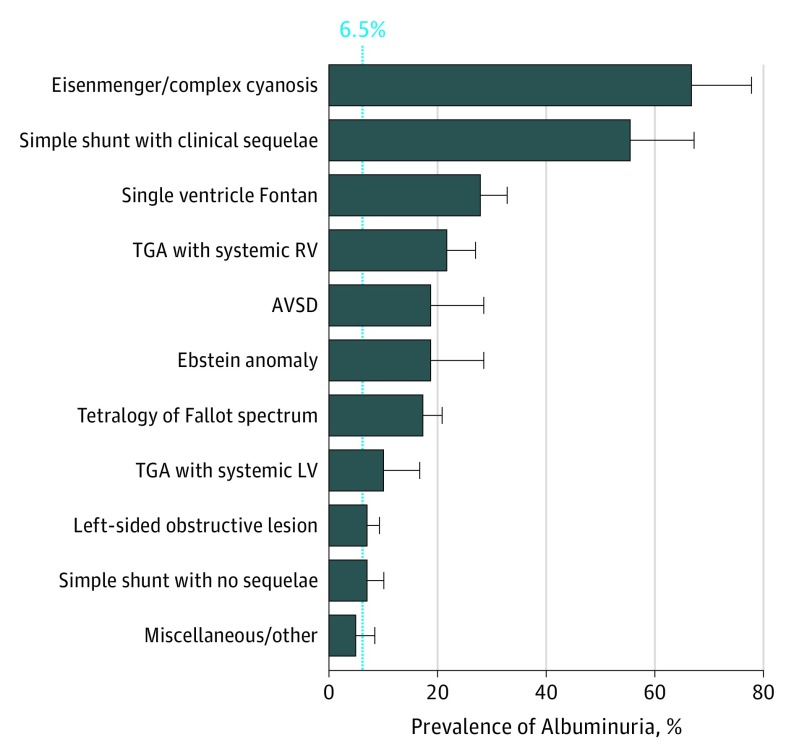
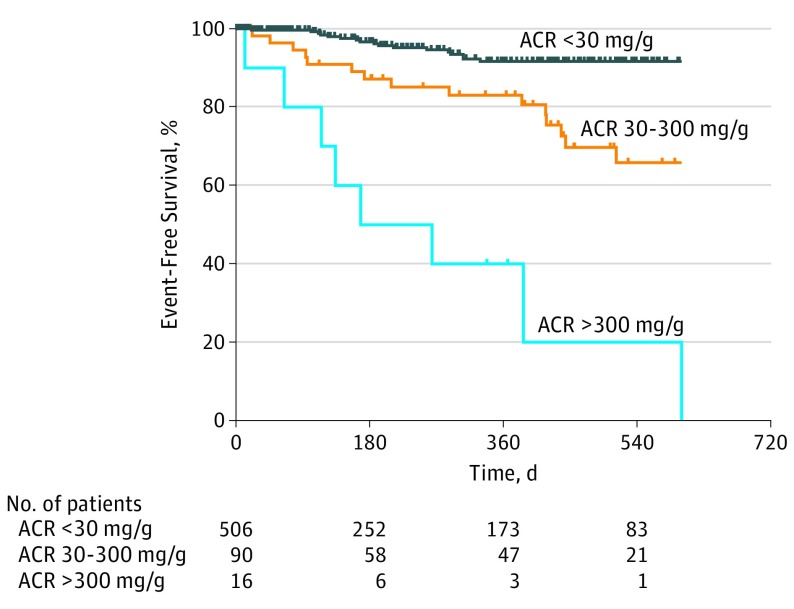
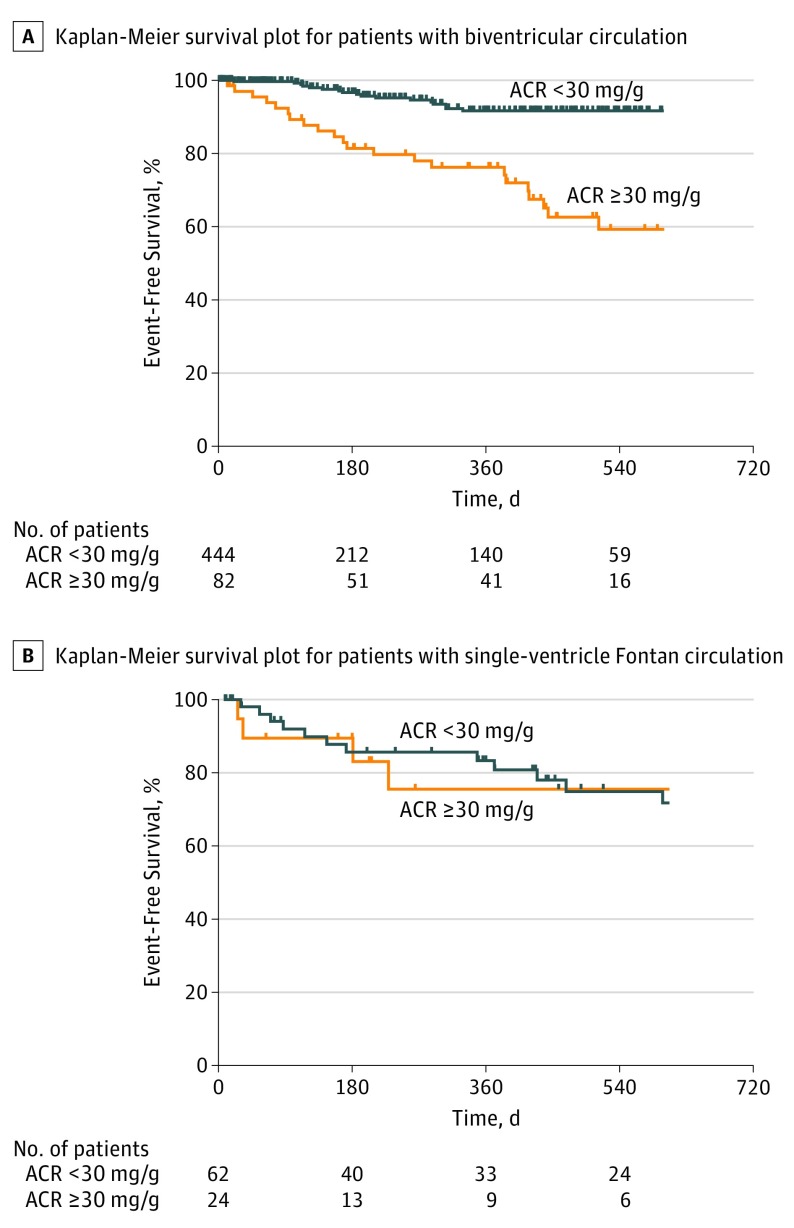
Results: We measured the ACR of 612 adult patients with CHD (mean [SD] age, 38.6 [13.4] years; 308 [50.3%] women). Albuminuria was present in 106 people (17.3%) and was associated with older age (patients with ACR <30 mg/g: mean [SD]: 37.5 [13.2] years; vs patients with ACR ≥30 mg/g: 43.8 [13.1] years; P < .001), presence of diabetes mellitus (ACR <30 mg/g: 13 of 506 [2.6%]; vs ≥30 mg/g: 11 of 106 [10.4%]; P < .001), lower estimated glomerular filtration rate (ACR <30 mg/g: median [interquartile range (IQR)]: 103.3 [90.0-116.4] mL/min/1.73 m2; ACR ≥30 mg/g: 99.1 [78.8-108.7] mL/min/1.73 m2; P = .002), and cyanosis (ACR <30 mg/g: 23 of 506 [5.1%]; vs ACR ≥30 mg/g: 21 of 106 [22.6%]; P < .001). After a mean (SD) follow-up time of 270 (288) days, 17 patients (2.5%) died, while 68 (11.1%) either died or experienced overnight inpatient admission. Albuminuria predicted outcome, with 30 of 106 patients with albuminuria (28.3%) affected vs 38 of 506 patients without albuminuria (7.5%; hazard ratio [HR], 3.0; 95% CI, 1.9-4.9; P < .001). Albuminuria was also associated with increased mortality (11 of 106 [10.4%]; vs 6 of 506 [1.2%] in patients with and without albuminuria, respectively; HR, 6.4; 95% CI, 2.4-17.3; P < .001). Albuminuria was associated with the outcomes only in patients with a biventricular circulation (HR, 4.5; 95% CI, 2.5-8.0) and not those with single-ventricle circulation (HR, 1.0; 95% CI, 0.4-2.8; P = 0.01 compared with biventricular circulation group). Among 133 patients (21.7%) in NYHA functional class 2, albuminuria was strongly associated with death or nonelective hospitalization.
Conclusions and relevance: Albuminuria is common and is associated with increased risk for adverse outcome in patients with ACHD with biventricular circulation. Albuminuria appears especially useful in stratifying risk in patients categorized as NYHA functional class 2.
Conflict of interest statement
Figures
Comment in
-
Association of Albuminuria With Outcomes in Adults With Congenital Heart Disease.JAMA Cardiol. 2018 Apr 1;3(4):316-317. doi: 10.1001/jamacardio.2018.0126. JAMA Cardiol. 2018. PMID: 29541743 No abstract available.
References
-
- O’Leary JM, Siddiqi OK, de Ferranti S, Landzberg MJ, Opotowsky AR. The changing demographics of congenital heart disease hospitalizations in the United States, 1998 through 2010. JAMA. 2013;309(10):984-986. - PubMed
-
- van der Bom T, Zomer AC, Zwinderman AH, Meijboom FJ, Bouma BJ, Mulder BJ. The changing epidemiology of congenital heart disease. Nat Rev Cardiol. 2011;8(1):50-60. - PubMed
-
- Opotowsky AR, Siddiqi OK, Webb GD. Trends in hospitalizations for adults with congenital heart disease in the U.S. J Am Coll Cardiol. 2009;54(5):460-467. - PubMed
-
- Jones CA, Francis ME, Eberhardt MS, et al. . Microalbuminuria in the US population: third National Health and Nutrition Examination Survey. Am J Kidney Dis. 2002;39(3):445-459. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
