

Association Between Hemodynamic Markers of Pulmonary Hypertension and Outcomes in Heart Failure With Preserved Ejection Fraction
- PMID: 29541759
- PMCID: PMC5875307
- DOI: 10.1001/jamacardio.2018.0128
Association Between Hemodynamic Markers of Pulmonary Hypertension and Outcomes in Heart Failure With Preserved Ejection Fraction
Erratum in
-
Error in Axis Label in Figures.JAMA Cardiol. 2018 Jul 1;3(7):665. doi: 10.1001/jamacardio.2018.1559. JAMA Cardiol. 2018. PMID: 29847612 Free PMC article. No abstract available.
Abstract
Importance: Heart failure with preserved ejection fraction (HFpEF) is highly prevalent, yet there are no specific therapies, possibly due to phenotypic heterogeneity. The development of pulmonary hypertension (PH) in patients with HFpEF is considered a high-risk phenotype in need of targeted therapies, but there have been limited hemodynamic and outcomes data.
Objective: To identify the hemodynamic characteristics and outcomes of PH-HFpEF.
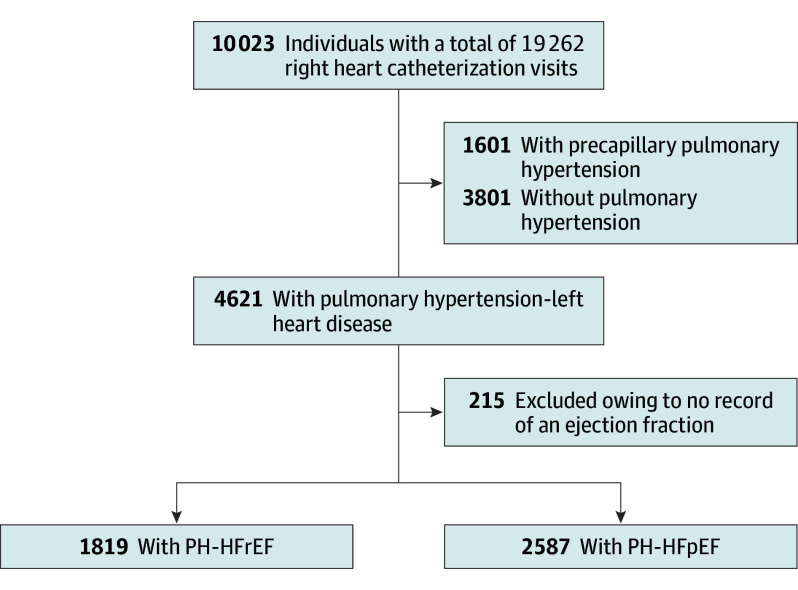
Design, setting, and participants: Cohort study of participants who had a right heart catheterization from January 2005 to September 2012 (median [interquartile range] follow-up time, 1578 [554-2513] days) were analyzed. Hemodynamic catheterization data was linked to the clinical data repository of all inpatient and outpatient encounters across a health system. Single tertiary referral center for heart failure and PH within a large health care network using a common clinical data repository was studied. There were 19 262 procedures in 10 023 participants.
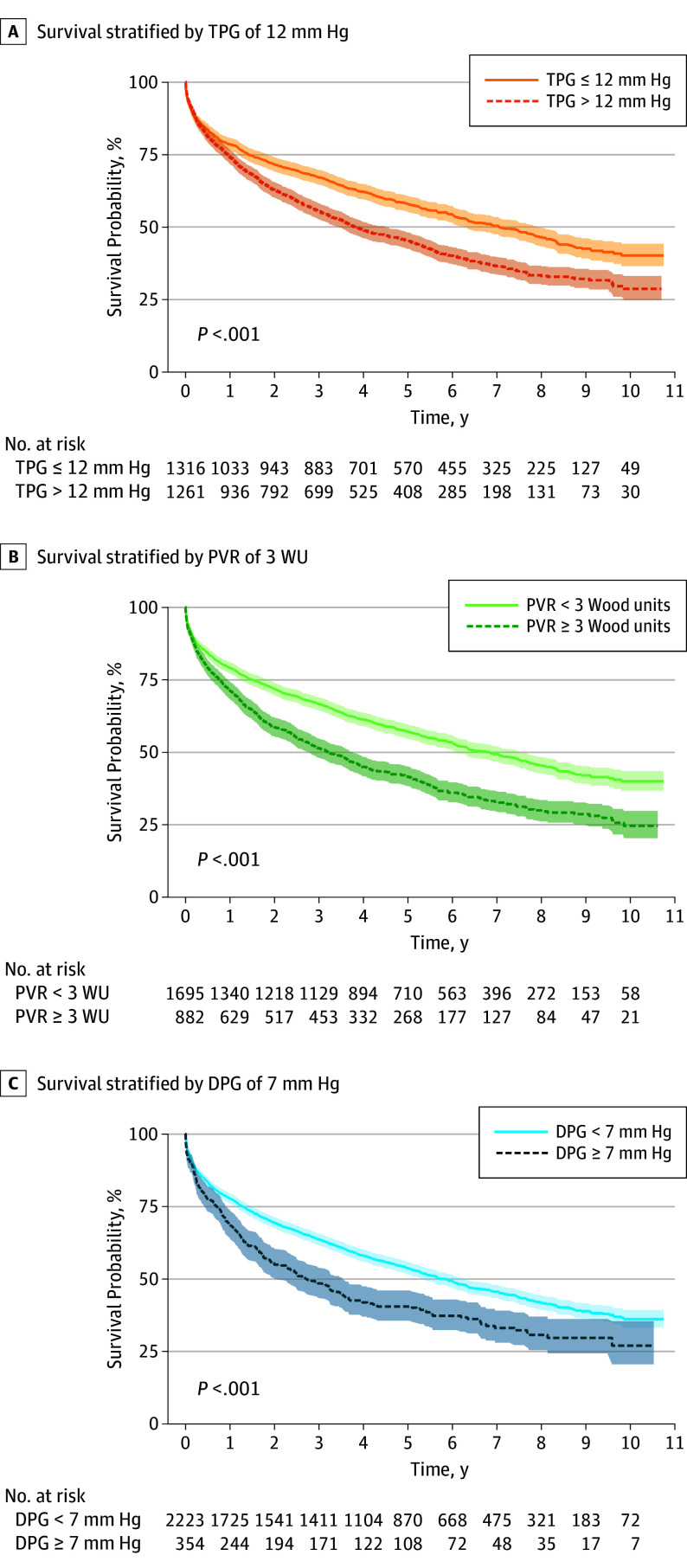
Exposures: Participants were classified as having no PH, precapillary PH, or PH in the setting of left heart disease (reduced or preserved ejection fraction). Pulmonary hypertension associated with HFpEF was defined as mean pulmonary artery pressure of 25 mm Hg or more, pulmonary artery wedge pressure of 15 mm Hg or more, and left ventricular ejection fraction of 45% or more. Pulmonary hypertension severity was quantified by the hemodynamic parameters transpulmonary gradient, pulmonary vascular resistance, and diastolic pulmonary gradient.
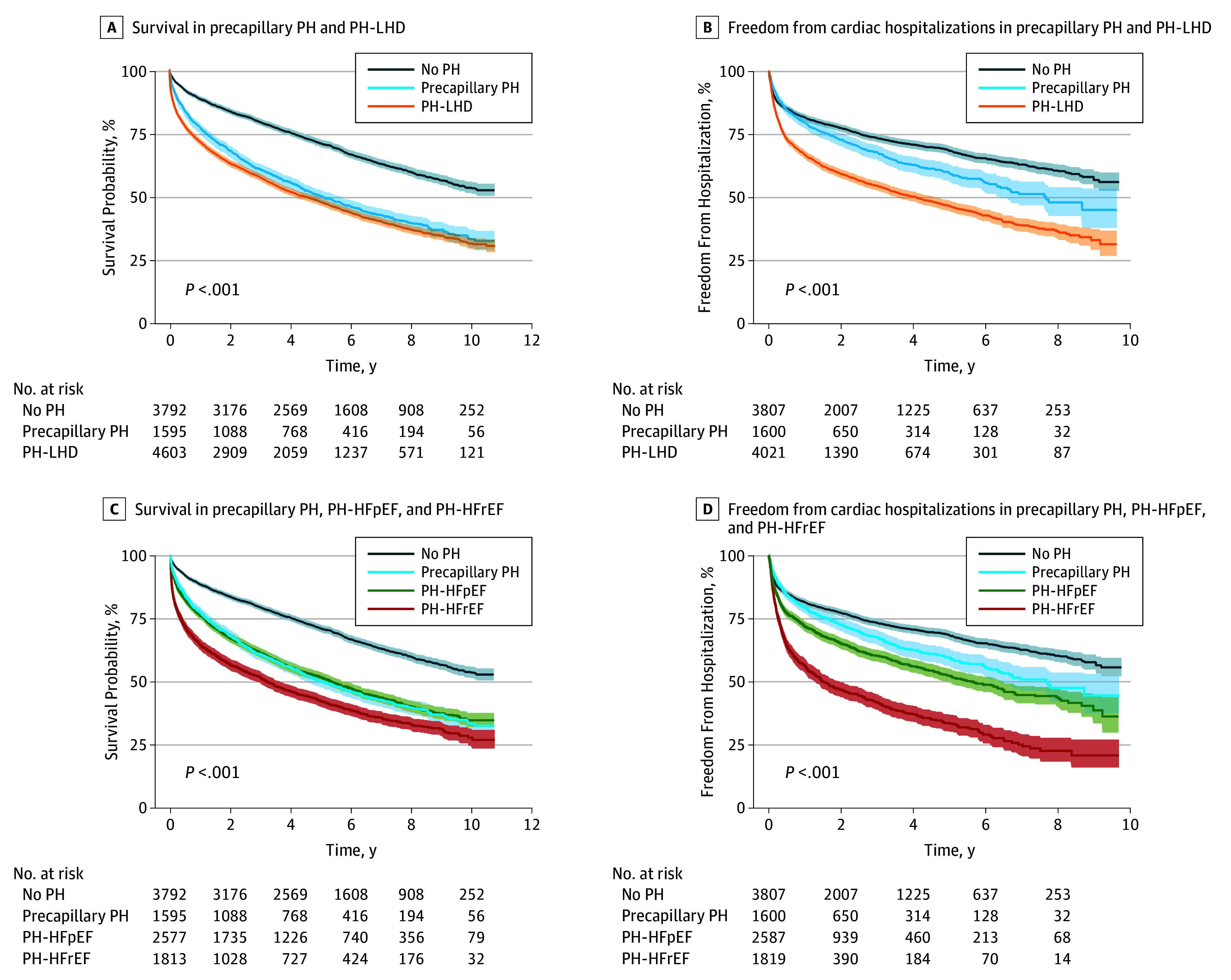
Main outcomes and measures: The primary outcome was time to all-cause mortality. Secondary outcomes were time to acute hospitalization and cardiovascular hospitalization.
Results: The mean (SD) of all study individuals was 65 (38) years. Of 10 023 individuals, 2587 (25.8%) had PH-HFpEF. Mortality was 23.6% at 1 year and 48.2% at 5 years. Cardiac hospitalizations occurred in 28.1% at 1 year and 47.4% at 5 years. The frequency of precapillary PH using clinically defined cut-offs for transpulmonary gradient (>12 mm Hg), pulmonary vascular resistance (3 Woods units), and diastolic pulmonary gradient (≥7 mm Hg) were 12.6%, 8.8%, and 3.5%, respectively. Transpulmonary gradient, pulmonary vascular resistance, and diastolic pressure gradient were predictive of mortality and cardiac hospitalizations.
Conclusions and relevance: In a large cohort referred for invasive hemodynamic assessment, PH-HFpEF was common. Transpulmonary gradient, pulmonary vascular resistance, and diastolic pulmonary gradient are all associated with mortality and cardiac hospitalizations.
Conflict of interest statement
Figures
Comment in
-
Population-Based Studies of Invasive Hemodynamics: A Glimpse Into the Future.JAMA Cardiol. 2018 Apr 1;3(4):306-307. doi: 10.1001/jamacardio.2018.0163. JAMA Cardiol. 2018. PMID: 29541741 No abstract available.
-
Left Ventricular Ejection Fraction Cut Point of 50% for Heart Failure With Preserved Ejection Fraction.JAMA Cardiol. 2018 Oct 1;3(10):1023. doi: 10.1001/jamacardio.2018.1906. JAMA Cardiol. 2018. PMID: 30027275 No abstract available.
-
Left Ventricular Ejection Fraction Cut Point of 50% for Heart Failure With Preserved Ejection Fraction-Reply.JAMA Cardiol. 2018 Oct 1;3(10):1023-1024. doi: 10.1001/jamacardio.2018.1936. JAMA Cardiol. 2018. PMID: 30027277 No abstract available.
References
-
- Go AS, Mozaffarian D, Roger VL, et al. ; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Executive summary: heart disease and stroke statistics: 2013 update: a report from the American Heart Association. Circulation. 2013;127(1):143-152. - PubMed
-
- Redfield MM, Jacobsen SJ, Burnett JC Jr, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289(2):194-202. - PubMed
-
- Bursi F, Weston SA, Redfield MM, et al. Systolic and diastolic heart failure in the community. JAMA. 2006;296(18):2209-2216. - PubMed
-
- Gerges C, Gerges M, Lang MB, et al. Diastolic pulmonary vascular pressure gradient: a predictor of prognosis in “out-of-proportion” pulmonary hypertension. Chest. 2013;143(3):758-766. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
