

Megestrol acetate for cachexia-anorexia syndrome. A systematic review
- PMID: 29542279
- PMCID: PMC5989756
- DOI: 10.1002/jcsm.12292
Megestrol acetate for cachexia-anorexia syndrome. A systematic review
Abstract
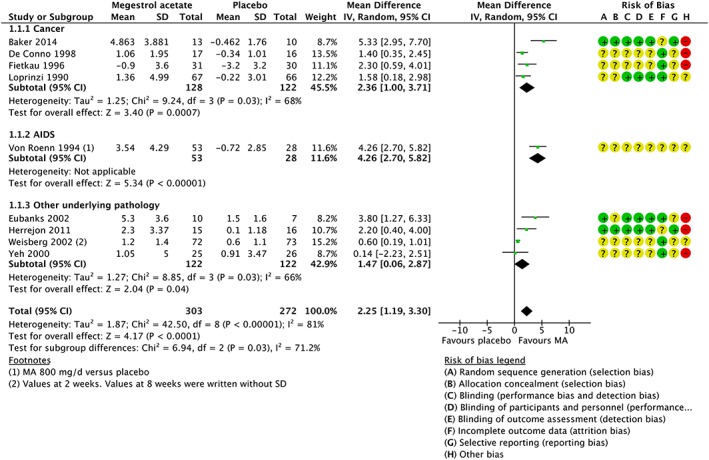
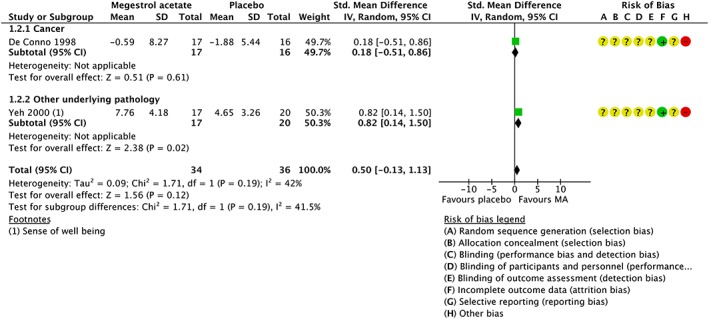
In 1993, megestrol acetate (MA) was approved by the US Food and Drug Administration for the treatment of anorexia, cachexia, or unexplained weight loss in patients with acquired immunodeficiency syndrome. The mechanism by which MA increases appetite is unknown, and its effectiveness for anorexia and cachexia in neoplastic, elderly, and acquired immunodeficiency syndrome patients is under investigation. This is an updated version of a Cochrane systematic review first published in 2005 and later updated in 2013 entitled 'Megestrol acetate for the treatment of anorexia-cachexia syndrome'. MA vs. placebo: in studies where MA was compared with placebo, the overall results showed that MA patients gained weight (mean difference, MD 2.25 kg, 95% CI [1.19, 3.3]) but did not gain quality of life (QOL) (standarized mean difference, SMD 0.5, 95% CI [-0.13, 1.13]), with more adverse events (relative risk, RR 1.46, 95% CI [1.05, 2.04]), but no difference in deaths (RR 1.26, 95% CI [0.70, 2.27]). MA vs. no treatment: MA patients gained weight (MD 1.45 kg, 95% CI [0.15, 2.75]) but did not gain QOL (standardized mean difference 3.89 95% CI [-14, 6.28]). There was no increase in adverse events (RR 0.90, 95% CI [0.39, 2.08]) or deaths (RR 1.01, 95% CI [0.42, 2.45]). MA vs. active drugs: MA patients gained weight (MD 2.5 kg, 95% CI [0.37, 4.64]) but did not gain QOL (MD 0.20 95% CI [-0.02, 0.43]) and did not report an increase in adverse events (RR 1.05 95% CI [0.95, 1.16]) or in deaths (RR 1.53, 95% CI [1.02, 2.29]) Different doses of MA: in studies where lower doses of MA were compared with higher doses of MA, we did not find differences either in weight gain (MD -0.94 kg, 95% CI [-3.33, 1.45]), QOL (MD 0.31 95% CI [-0.19, 0.81]), or adverse events (RR 1.34, 95% CI [0.65, 2.76]). Thus, we cannot reach a conclusion for an optimal dose of MA.
Keywords: Anorexia; Appetite Stimulants; Cachexia; Megestrol Acetate; Randomized Controlled Trials; Systematic Review.
© 2018 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of the Society on Sarcopenia, Cachexia and Wasting Disorders.
Figures
Similar articles
-
Dose-dependent effect of megestrol acetate supplementation in cancer patients with anorexia-cachexia syndrome: A meta-analysis.J Cachexia Sarcopenia Muscle. 2024 Aug;15(4):1254-1263. doi: 10.1002/jcsm.13500. Epub 2024 Jun 20. J Cachexia Sarcopenia Muscle. 2024. PMID: 39031821 Free PMC article. Review.
-
Usage of megestrol acetate in the treatment of anorexia-cachexia syndrome in the elderly.J Nutr Health Aging. 2009 May;13(5):448-54. doi: 10.1007/s12603-009-0082-1. J Nutr Health Aging. 2009. PMID: 19390752 Clinical Trial.
-
The effect of megestrol acetate on anorexia, weight loss and cachexia in cancer and AIDS patients (review).Anticancer Res. 1997 Jan-Feb;17(1B):657-62. Anticancer Res. 1997. PMID: 9066597 Review.
-
Anticachectic efficacy of megestrol acetate at different doses and versus placebo in patients with neoplastic cachexia.Am J Clin Oncol. 1998 Aug;21(4):347-51. doi: 10.1097/00000421-199808000-00006. Am J Clin Oncol. 1998. PMID: 9708631 Clinical Trial.
-
Systematic review of megestrol acetate in the treatment of anorexia-cachexia syndrome.J Pain Symptom Manage. 2004 Apr;27(4):360-9. doi: 10.1016/j.jpainsymman.2003.09.007. J Pain Symptom Manage. 2004. PMID: 15050664
Cited by
-
Unlocking Prognostic Genes and Multi-Targeted Therapeutic Bioactives from Herbal Medicines to Combat Cancer-Associated Cachexia: A Transcriptomics and Network Pharmacology Approach.Int J Mol Sci. 2023 Dec 21;25(1):156. doi: 10.3390/ijms25010156. Int J Mol Sci. 2023. PMID: 38203330 Free PMC article.
-
Dose-dependent effect of megestrol acetate supplementation in cancer patients with anorexia-cachexia syndrome: A meta-analysis.J Cachexia Sarcopenia Muscle. 2024 Aug;15(4):1254-1263. doi: 10.1002/jcsm.13500. Epub 2024 Jun 20. J Cachexia Sarcopenia Muscle. 2024. PMID: 39031821 Free PMC article. Review.
-
Supportive care of female hormones in brain health: what and how?Front Pharmacol. 2024 Jul 24;15:1403969. doi: 10.3389/fphar.2024.1403969. eCollection 2024. Front Pharmacol. 2024. PMID: 39114348 Free PMC article. Review.
-
Mirtazapine versus Megestrol in the Treatment of Anorexia-Cachexia Syndrome in Patients with Advanced Cancer: A Randomized, Double-Blind, Controlled Phase II Clinical Trial.Cancers (Basel). 2023 Jul 12;15(14):3588. doi: 10.3390/cancers15143588. Cancers (Basel). 2023. PMID: 37509249 Free PMC article.
-
Clinical efficacy and safety evaluation of Buzhongyiqi pills on appetite improvement in patients with colorectal cancer receiving chemotherapy: a pilot randomized cross-over clinical trial.J Tradit Chin Med. 2024 Dec;44(6):1254-1267. doi: 10.19852/j.cnki.jtcm.20240806.005. J Tradit Chin Med. 2024. PMID: 39617711 Free PMC article. Clinical Trial.
References
-
- Berenstein EG, Ortiz Z. Megestrol acetate for the treatment of anorexia‐cachexia syndrome. Cochrane Database Syst Rev 2003. - PubMed
-
- Berenstein EG, Ortiz Z. Megestrol acetate for the treatment of anorexia‐cachexia syndrome. Cochrane Database Syst Rev 2005. - PubMed
-
- Nelson KA, Walsh D, Sheehan FA. The cancer anorexia‐cachexia syndrome. J Clin Oncol 1994;12:213–225. - PubMed
-
- Splinter TA. Cachexia and cancer: a clinician's view. Ann Oncol Off J Eur Soc Med Oncol ESMO 1992;3:25–27. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
