

Geographic Variations in Arthritis Prevalence, Health-Related Characteristics, and Management - United States, 2015
- PMID: 29543787
- PMCID: PMC5857191
- DOI: 10.15585/mmwr.ss6704a1
Geographic Variations in Arthritis Prevalence, Health-Related Characteristics, and Management - United States, 2015
Abstract
Problem/condition: Doctor-diagnosed arthritis is a common chronic condition affecting an estimated 23% (54 million) of adults in the United States, greatly influencing quality of life and costing approximately $300 billion annually. The geographic variations in arthritis prevalence, health-related characteristics, and management among states and territories are unknown. Therefore, public health professionals need to understand arthritis in their areas to target dissemination of evidence-based interventions that reduce arthritis morbidity.
Reporting period: 2015.
Description of system: The Behavioral Risk Factor Surveillance System is an annual, random-digit-dialed landline and cellular telephone survey of noninstitutionalized adults aged ≥18 years residing in the United States. Self-reported data are collected from the 50 states, the District of Columbia, Guam, and Puerto Rico. Unadjusted and age-standardized prevalences of arthritis, arthritis health-related characteristics, and arthritis management were calculated. County-level estimates were calculated using a validated statistical modeling method.
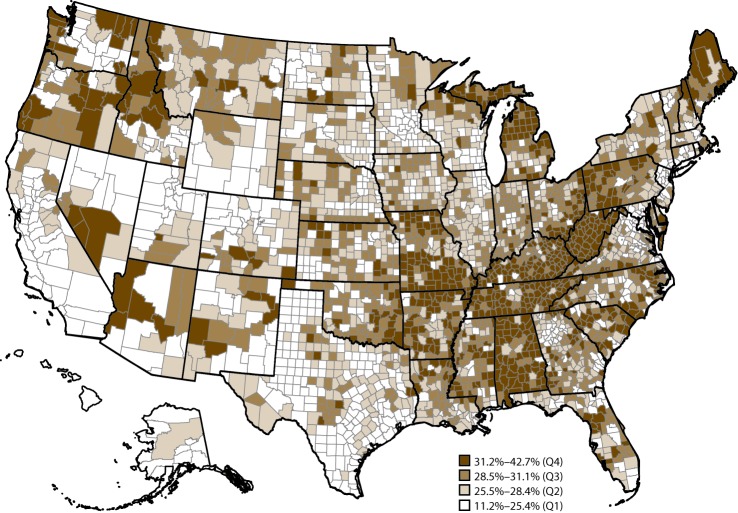
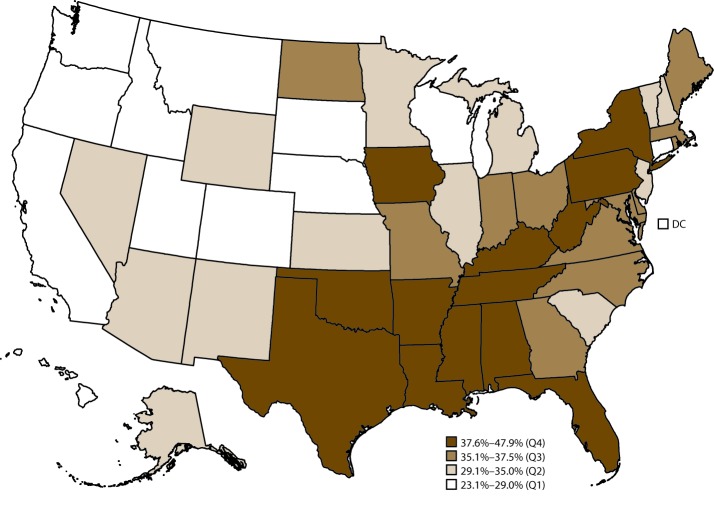
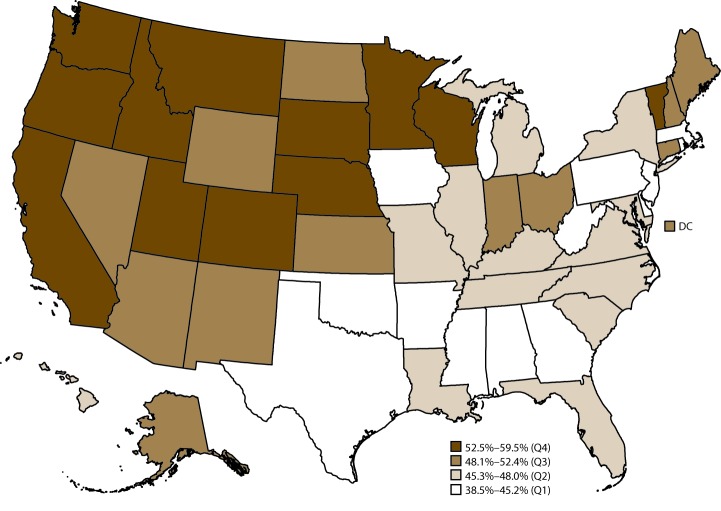
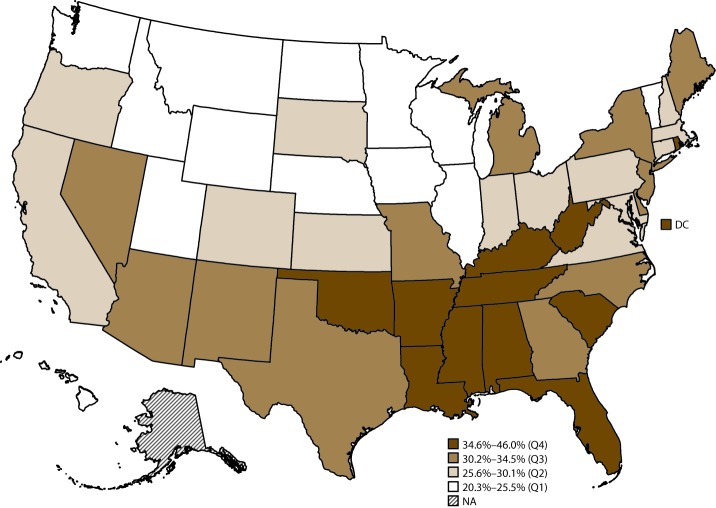
Results: In 2015, in the 50 states and the District of Columbia, median age-standardized prevalence of arthritis was 23.0% (range: 17.2%-33.6%). Modeled prevalence of arthritis varied considerably by county (range: 11.2%-42.7%). In 13 states that administered the arthritis management module, among adults with arthritis, the age-standardized median percentage of participation in a self-management education course was 14.5% (range: 9.1%-19.0%), being told by a health care provider to engage in physical activity or exercise was 58.5% (range: 52.3%-61.9%), and being told to lose weight to manage arthritis symptoms (if overweight or obese) was 44.5% (range: 35.1%-53.2%). Respondents with arthritis who lived in the quartile of states with the highest prevalences of arthritis had the highest percentages of negative health-related characteristics (i.e., arthritis-attributable activity limitations, arthritis-attributable severe joint pain, and arthritis-attributable social participation restriction; ≥14 physically unhealthy days during the past 30 days; ≥14 mentally unhealthy days during the past 30 days; obesity; and leisure-time physical inactivity) and the lowest percentage of leisure-time walking.
Interpretation: The prevalence, health-related characteristics, and management of arthritis varied substantially across states. The modeled prevalence of arthritis varied considerably by county.
Public health action: The findings highlight notable geographic variability in prevalence, health-related characteristics, and management of arthritis. Targeted use of evidence-based interventions that focus on physical activity and self-management education can reduce pain and improve function and quality of life for adults with arthritis and thus might reduce these geographic disparities.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous