

From somatic variants towards precision oncology: Evidence-driven reporting of treatment options in molecular tumor boards
- PMID: 29544535
- PMCID: PMC5856211
- DOI: 10.1186/s13073-018-0529-2
From somatic variants towards precision oncology: Evidence-driven reporting of treatment options in molecular tumor boards
Abstract
Background: A comprehensive understanding of cancer has been furthered with technological improvements and decreasing costs of next-generation sequencing (NGS). However, the complexity of interpreting genomic data is hindering the implementation of high-throughput technologies in the clinical context: increasing evidence on gene-drug interactions complicates the task of assigning clinical significance to genomic variants.
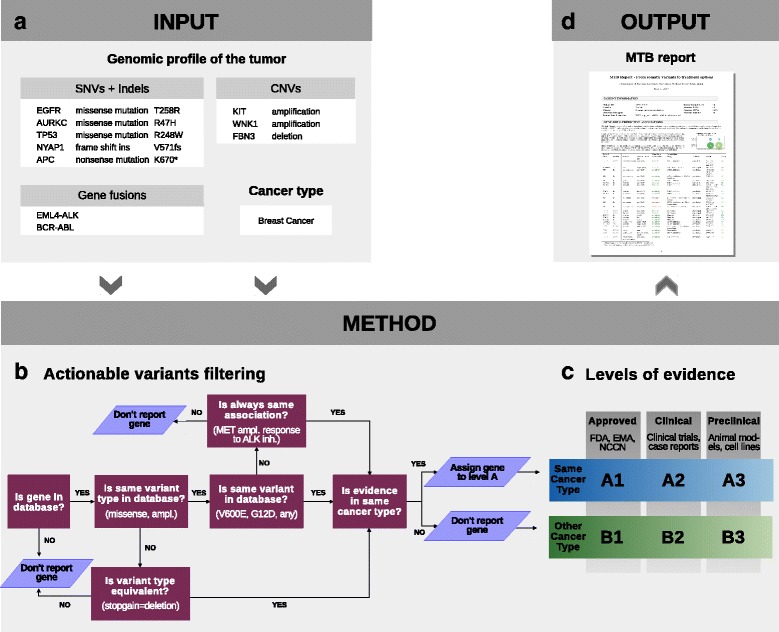
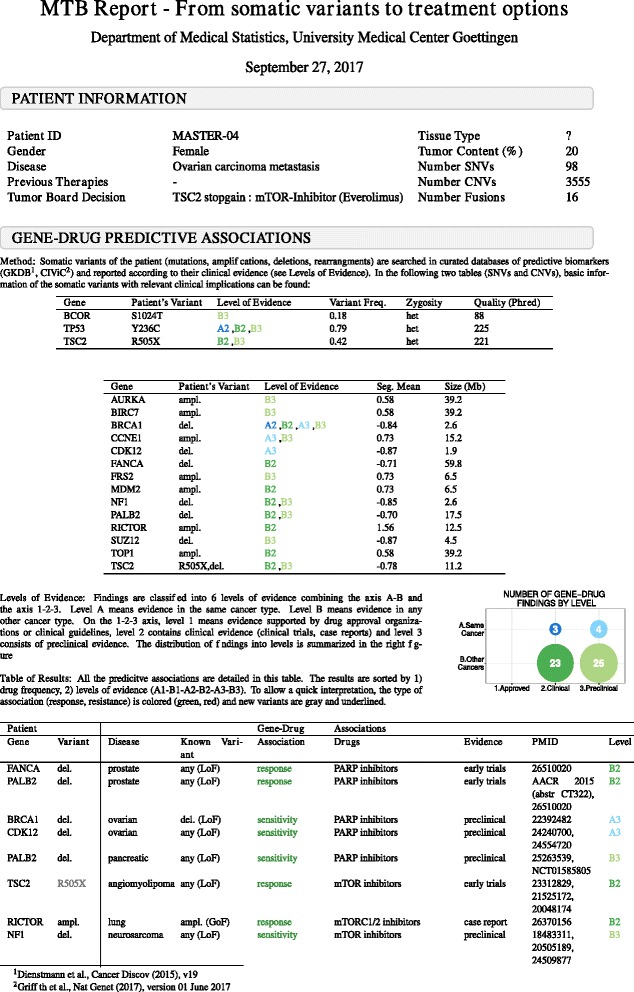
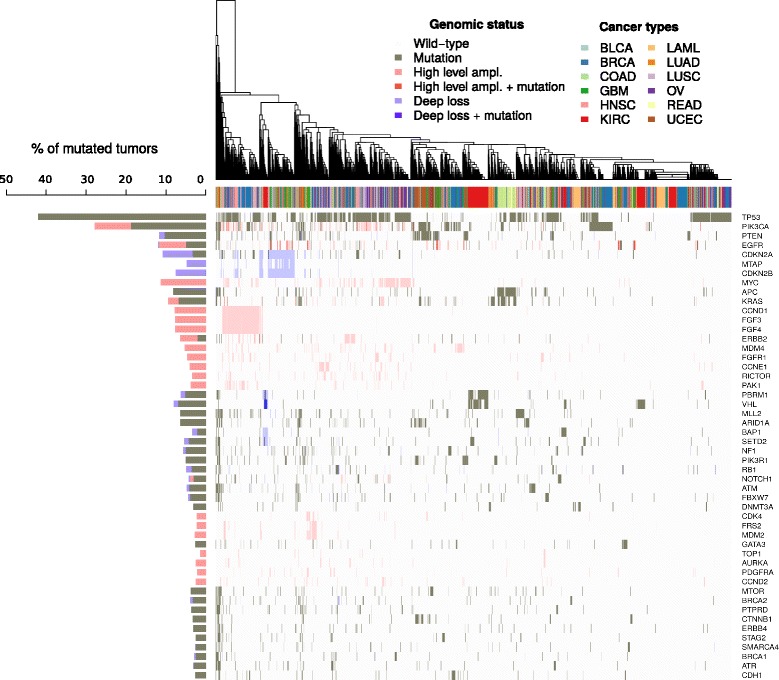
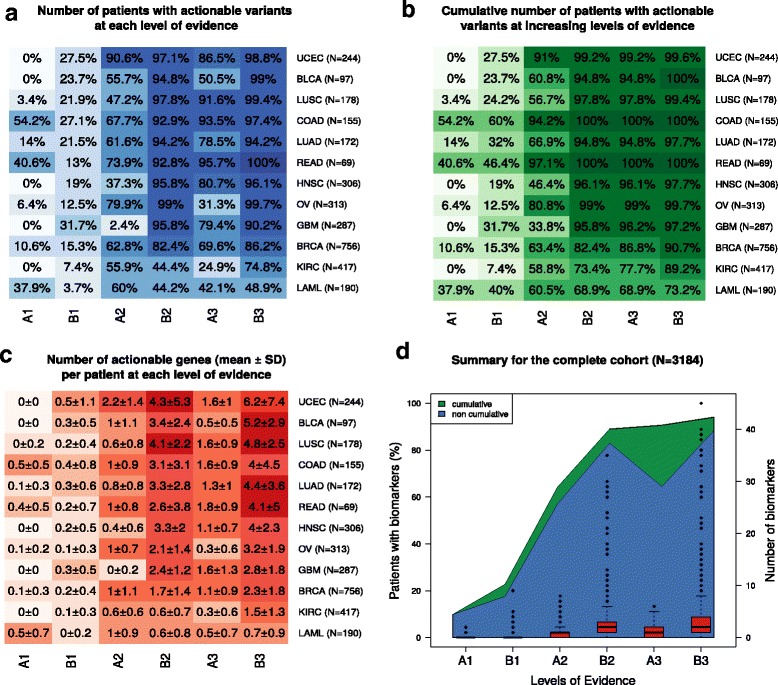
Methods: Here we present a method that automatically matches patient-specific genomic alterations to treatment options. The method relies entirely on public knowledge of somatic variants with predictive evidence on drug response. The output report is aimed at supporting clinicians in the task of finding the clinical meaning of genomic variants. We applied the method to 1) The Cancer Genome Atlas (TCGA) and Genomics Evidence Neoplasia Information Exchange (GENIE) cohorts and 2) 11 patients from the NCT MASTER trial whose treatment discussions included information on their genomic profiles.
Results: Our reporting strategy showed a substantial number of patients with actionable variants in the analyses of TCGA and GENIE samples. Notably, it was able to reproduce experts' treatment suggestions in a retrospective study of 11 patients from the NCT MASTER trial. Our results establish a proof of concept for comprehensive, evidence-based reports as a supporting tool for discussing treatment options in tumor boards.
Conclusions: We believe that a standardized method to report actionable somatic variants will smooth the incorporation of NGS in the clinical context. We anticipate that tools like the one we present here will become essential in summarizing for clinicians the growing evidence in the field of precision medicine. The R code of the presented method is provided in Additional file 6 and available at https://github.com/jperera-bel/MTB-Report .
Keywords: Actionable variants; Cancer genomics; Genomic report; Molecular tumor board; Personalized treatment; Predictive biomarkers; Targeted therapies.
Conflict of interest statement
Ethics approval and consent to participate
All patient data were obtained following written informed consent under the NCT MASTER trial, an institutional review board-approved clinical sequencing program for younger patients with advanced-stage hematological and oncological diseases across all malignancies. The trial protocol was approved by the Ethics Committee of Heidelberg University. Research within NCT MASTER was conducted in accordance with the Declaration of Helsinki.
Consent for publication
Written informed consent for publication was obtained under the NCT MASTER trial.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Center for Drug Evaluation and Research. Genomics - Table of Pharmacogenomic Biomarkers in Drug Labeling. https://www.fda.gov/Drugs/ScienceResearch/ResearchAreas/Pharmacogenetics.... Accessed 6 Mar 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
