

MAGIC biomarkers predict long-term outcomes for steroid-resistant acute GVHD
- PMID: 29545329
- PMCID: PMC6014357
- DOI: 10.1182/blood-2018-01-822957
MAGIC biomarkers predict long-term outcomes for steroid-resistant acute GVHD
Abstract
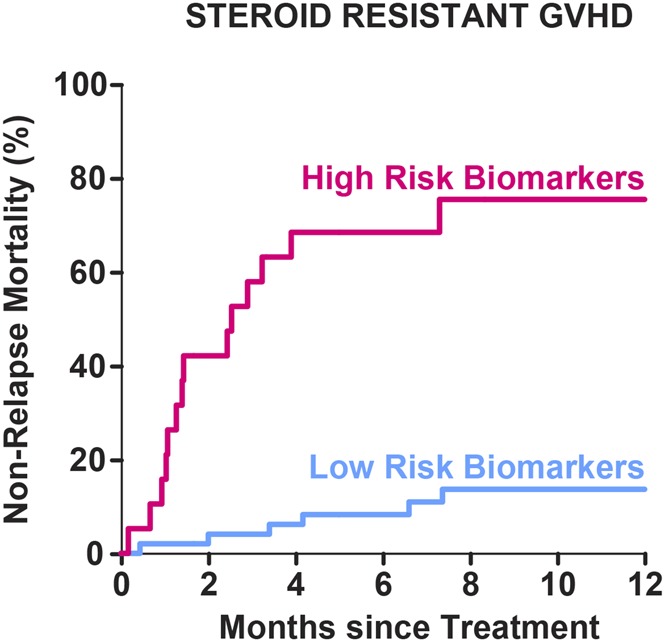
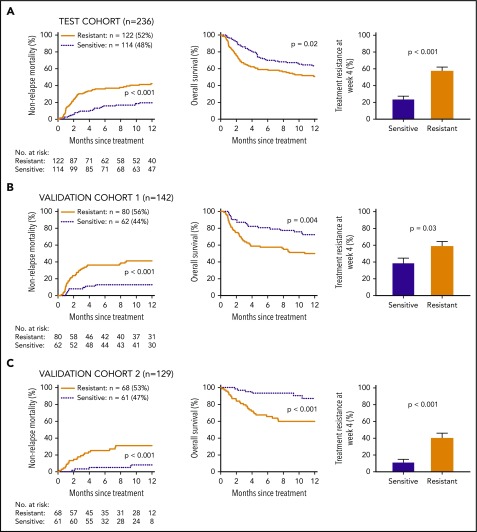
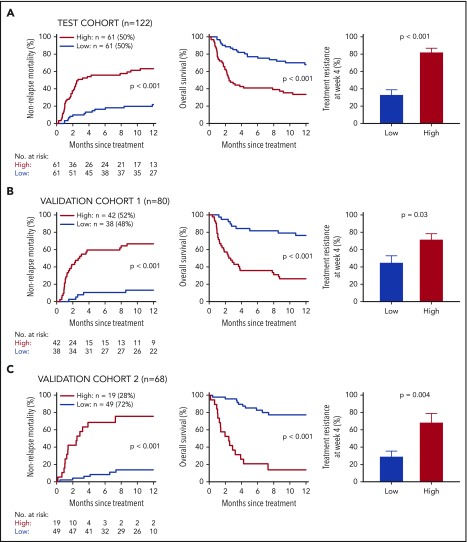
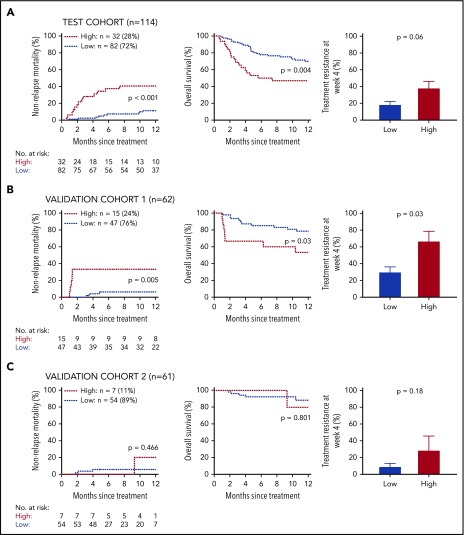
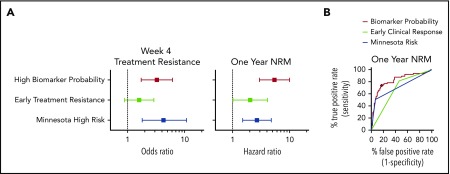
Acute graft-versus-host disease (GVHD) is treated with systemic corticosteroid immunosuppression. Clinical response after 1 week of therapy often guides further treatment decisions, but long-term outcomes vary widely among centers, and more accurate predictive tests are urgently needed. We analyzed clinical data and blood samples taken 1 week after systemic treatment of GVHD from 507 patients from 17 centers of the Mount Sinai Acute GVHD International Consortium (MAGIC), dividing them into a test cohort (n = 236) and 2 validation cohorts separated in time (n = 142 and n = 129). Initial response to systemic steroids correlated with response at 4 weeks, 1-year nonrelapse mortality (NRM), and overall survival (OS). A previously validated algorithm of 2 MAGIC biomarkers (ST2 and REG3α) consistently separated steroid-resistant patients into 2 groups with dramatically different NRM and OS (P < .001 for all 3 cohorts). High biomarker probability, resistance to steroids, and GVHD severity (Minnesota risk) were all significant predictors of NRM in multivariate analysis. A direct comparison of receiver operating characteristic curves showed that the area under the curve for biomarker probability (0.82) was significantly greater than that for steroid response (0.68, P = .004) and for Minnesota risk (0.72, P = .005). In conclusion, MAGIC biomarker probabilities generated after 1 week of systemic treatment of GVHD predict long-term outcomes in steroid-resistant GVHD better than clinical criteria and should prove useful in developing better treatment strategies.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: J.E.L., J.L.M.F., and U.Ö. are joint inventors on a GVHD biomarker patent. The remaining authors declare no competing financial interests.
Figures
References
-
- MacMillan ML, DeFor TE, Weisdorf DJ. The best endpoint for acute GVHD treatment trials. Blood. 2010;115(26):5412-5417. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
