

Clinical Characteristics and Etiology of Bilateral Vestibular Loss in a Cohort from Central Illinois
- PMID: 29545765
- PMCID: PMC5837982
- DOI: 10.3389/fneur.2018.00046
Clinical Characteristics and Etiology of Bilateral Vestibular Loss in a Cohort from Central Illinois
Abstract
Background: Previous series of bilateral vestibular loss (BVL) identified numerous etiologies, but surprisingly, a cause in a significant number of cases remains unknown. In an effort to understand possible etiology and management strategies, a global effort is currently in progress. Here, I contribute my 10-year experience with both acute and chronic BVL during the 2007-2017 decade.
Methods: This is a retrospective review of the charts and EMR of patients diagnosed with BVL in the last 10 years. Following Institutional IRB approval, we identified 57 patients with a diagnosis of BVL and utilized the current diagnostic criteria listed by the Barany society (1). The inclusion criteria included patients with BVL of any cause, within an age span older than 18 and a neuro-otologic examination supporting the clinical impression of BVL.
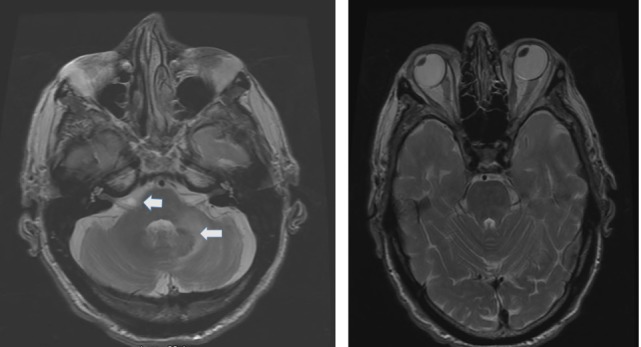
Results: During the current decade 2007-2017, I identified two broad categories of BVL (acute and chronic) in 57 patients; only 41 of them had records available. The etiology includes: idiopathic: n = 9, Wernicke's encephalopathy n = 11, superficial siderosis n = 3, paraneoplastic syndrome: n = 3, bilateral vestibular neuritis (recurrent AVS lasting days without cochlear symptoms) n = 3, simultaneous ototoxicity of aminoglycoside and chemotherapy toxicity n = 2, MELAS n = 2, Meniere's disease treated with intra-tympanic streptomycin in one ear n = 1, acute phenytoin intoxication: n = 1, combined chronic unilateral tumor-related vestibulopathy and new contralateral vestibular neuritis (this patient presented with Betcherew's phenomenon) n = 1, bilateral AICA stroke n = 1, mixed spinocerebellar ataxia type 3, n = 2 and CANVAS n = 2.
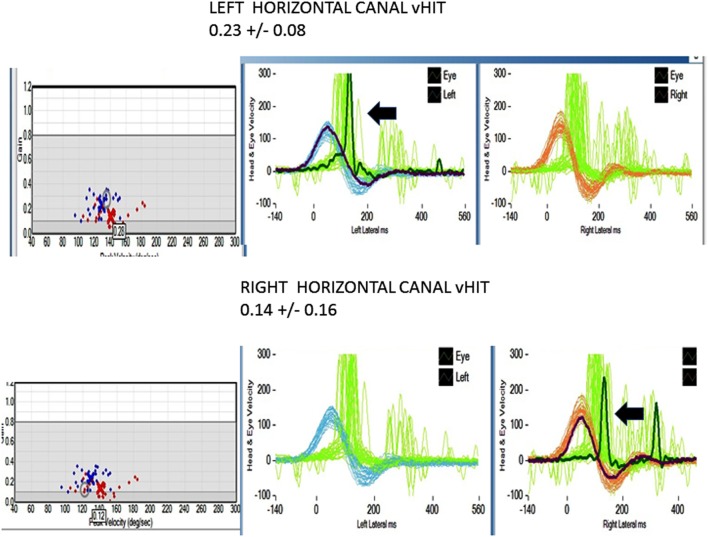
Conclusion: This cohort included a 28% overall incidence of acute and subacute BVL; among them, 65% improved with intervention. In the thiamine deficiency group, specifically, the vestibular function improved in 80% of the patients. Even though acute, subacute, or chronic showed slightly asymmetric horizontal-VOR gain loss, it never did cause spontaneous, primary straight gaze horizontal nystagmus. n = 39/41 patients had abnormal manual HIT, n = 26/41 BVL patients tested with video head impulse immediately after manual testing showed decreased VOR gain, including two with covert saccades. Two thiamine patients with positive bedside pretreatment manual HIT, tested after treatment with high-dose thiamine showed improved VOR. In acute thiamine deficiency, the horizontal VOR was abnormal and the vertical was either normal or mildly decreased. This series favored a neurologic cause of BVL. Finally, 20% of the chronic cases were idiopathic.
Keywords: acute bilateral vestibular loss; bilateral vestibulopathy; chronic bilateral; neurologic disorders associated with bilateral vestibular loss; vestibular loss.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources