

Current diagnostic imaging of pheochromocytomas and implications for therapeutic strategy
- PMID: 29545830
- PMCID: PMC5840941
- DOI: 10.3892/etm.2018.5871
Current diagnostic imaging of pheochromocytomas and implications for therapeutic strategy
Abstract
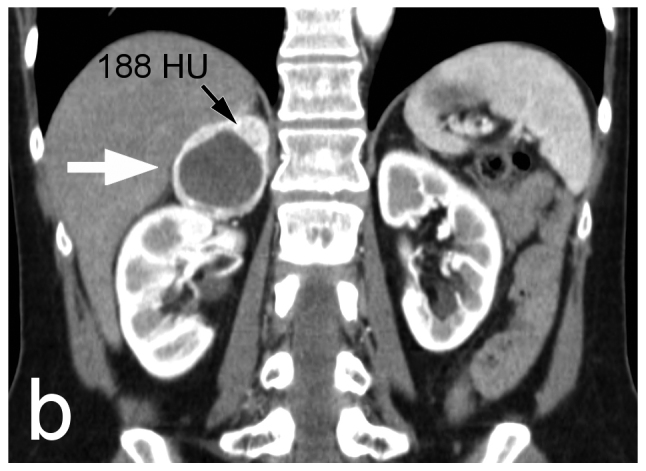
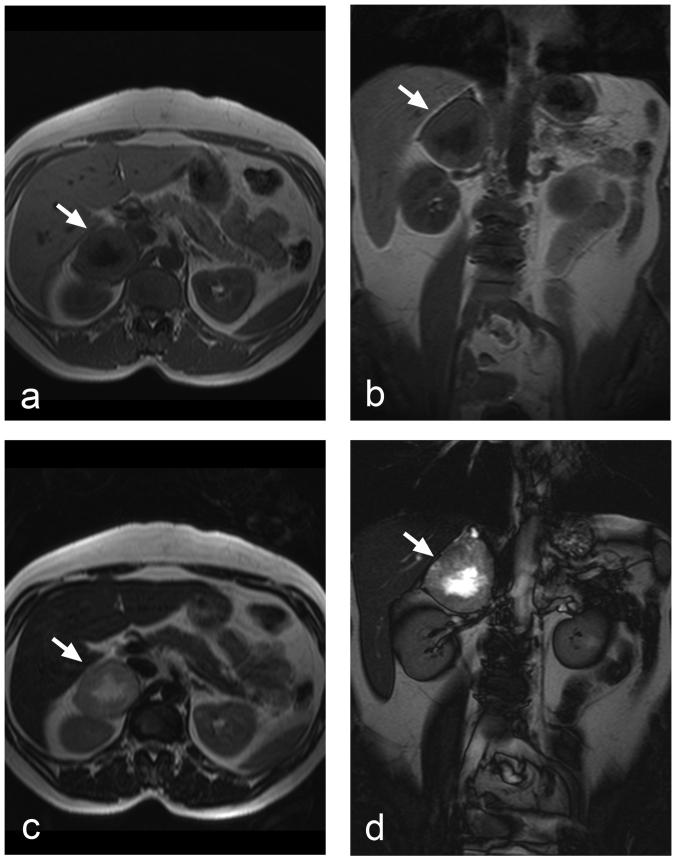
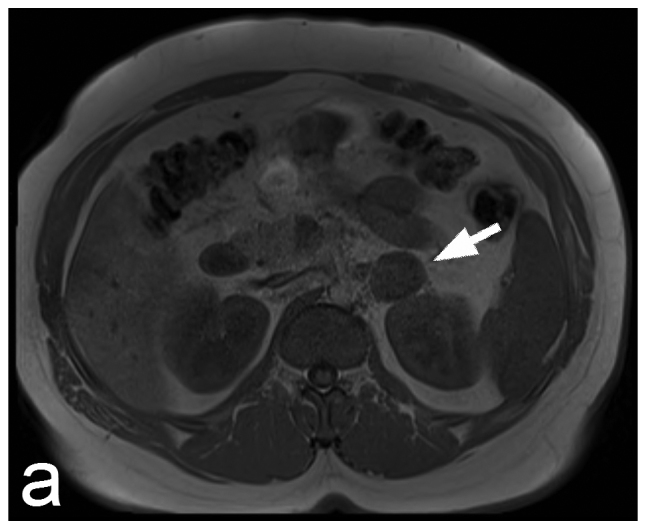
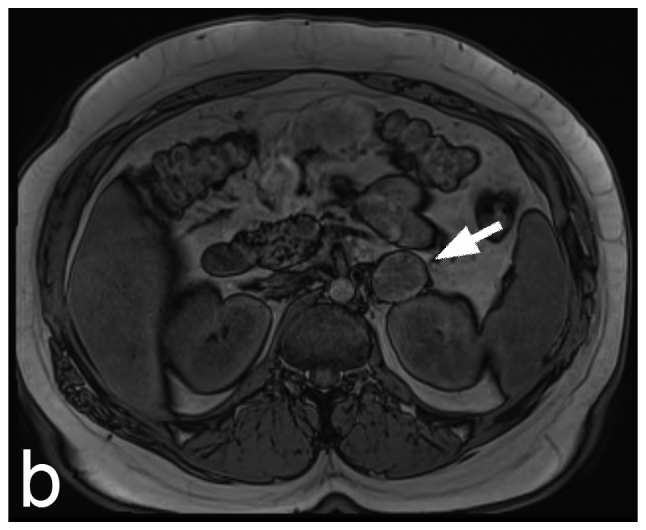
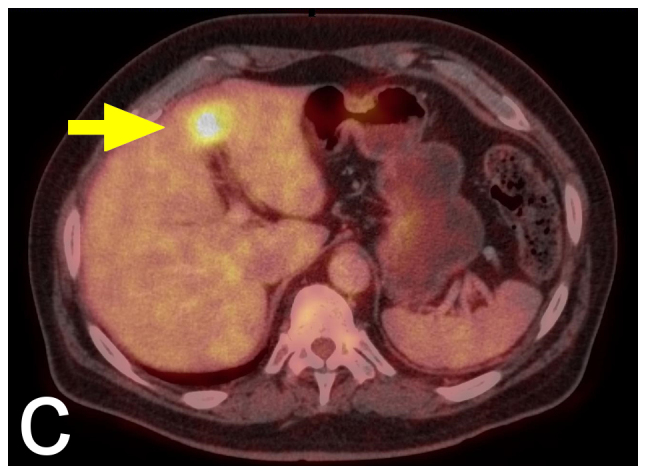
The topic of pheochromocytomas is becoming increasingly popular as a result of major advances in different medical fields, including laboratory diagnosis, genetics, therapy, and particularly in novel advances in imaging techniques. The present review article discusses current clinical, biochemical, genetic and histopathological aspects of the diagnosis of pheochromocytomas and planning of pre-surgical preparation and subsequent surgical treatment options. The main part of the paper is focused on the role of morphological imaging methods (primarily computed tomography and magnetic resonance imaging) and functional imaging (scintigraphy and positron emission tomography) in the diagnosis and staging of pheochromocytomas.
Keywords: adrenal masses; adrenalectomy; imaging; incidentalomas; pheochromocytoma.
Figures
Similar articles
-
Pheochromocytoma: presentation, diagnosis and treatment.J Hypertens. 2006 Dec;24(12):2331-9. doi: 10.1097/01.hjh.0000251887.01885.54. J Hypertens. 2006. PMID: 17082709 Review.
-
6-18F-fluoro-L-dihydroxyphenylalanine positron emission tomography is superior to 123I-metaiodobenzyl-guanidine scintigraphy in the detection of extraadrenal and hereditary pheochromocytomas and paragangliomas: correlation with vesicular monoamine transporter expression.J Clin Endocrinol Metab. 2010 Jun;95(6):2800-10. doi: 10.1210/jc.2009-2352. Epub 2010 Apr 6. J Clin Endocrinol Metab. 2010. PMID: 20371665
-
Quantitative analysis of normal and pathologic adrenal glands with 18F-FDOPA PET/CT: focus on pheochromocytomas.Nucl Med Commun. 2017 Sep;38(9):771-779. doi: 10.1097/MNM.0000000000000708. Nucl Med Commun. 2017. PMID: 28704339
-
Advances in the diagnosis and therapy of adrenal tumors.Curr Opin Oncol. 1998 Jan;10(1):52-7. doi: 10.1097/00001622-199801000-00009. Curr Opin Oncol. 1998. PMID: 9466485 Review.
-
Management of incidentally discovered adrenal masses.World J Urol. 1999 Feb;17(1):9-14. doi: 10.1007/s003450050098. World J Urol. 1999. PMID: 10096145 Review.
Cited by
-
An Aberrant Case of Pheochromocytoma in a Young Adult Presenting With Secondary Hypertension: A Case Report With Review of the Literature.Cureus. 2023 Sep 8;15(9):e44891. doi: 10.7759/cureus.44891. eCollection 2023 Sep. Cureus. 2023. PMID: 37814748 Free PMC article.
-
Synchronized Laparoscopic Bilateral Adrenalectomy for Pheochromocytoma in Multiple Endocrine Neoplasia Syndrome: A Case Report.J Kidney Cancer VHL. 2022 Sep 2;9(3):24-28. doi: 10.15586/jkcvhl.v9i3.239. eCollection 2022. J Kidney Cancer VHL. 2022. PMID: 36132070 Free PMC article.
-
Effects of pretreatment with terazosin and valsartan on intraoperative haemodynamics in patients with phaeochromocytoma.Eur J Hosp Pharm. 2022 Jul;29(4):192-197. doi: 10.1136/ejhpharm-2020-002375. Epub 2020 Sep 7. Eur J Hosp Pharm. 2022. PMID: 32895230 Free PMC article.
-
Diagnostic Value of Unenhanced CT Attenuation and CT Histogram Analysis in Differential Diagnosis of Adrenal Tumors.Medicina (Kaunas). 2020 Nov 9;56(11):597. doi: 10.3390/medicina56110597. Medicina (Kaunas). 2020. PMID: 33182333 Free PMC article.
-
Global epidemiology of pheochromocytoma: a systematic review and meta-analysis of observational studies.J Endocrinol Invest. 2025 Jul 2. doi: 10.1007/s40618-025-02639-9. Online ahead of print. J Endocrinol Invest. 2025. PMID: 40601232 Review.
References
-
- Lloyd RV, Osamura RY, Klöppel G, Rosai J. WHO Classification of Tumours of Endocrine Organs. 4th. IACR; Lyon: 2017.
LinkOut - more resources
Full Text Sources
Other Literature Sources