

Modified Blumgart anastomosis without pancreatic duct-to-jejunum mucosa anastomosis for pancreatoduodenectomy: a feasible and safe novel technique
- PMID: 29545971
- PMCID: PMC5842338
- DOI: 10.20892/j.issn.2095-3941.2017.0153
Modified Blumgart anastomosis without pancreatic duct-to-jejunum mucosa anastomosis for pancreatoduodenectomy: a feasible and safe novel technique
Abstract
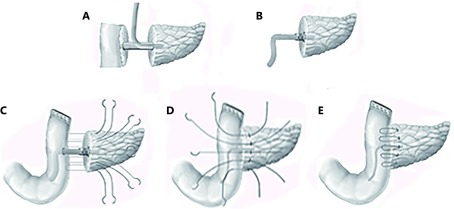
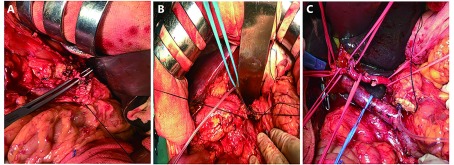
Objective: This study proposed a modified Blumgart anastomosis (m-BA) that uses a firm ligation of the main pancreatic duct with a supporting tube to replace the pancreatic duct-to-jejunum mucosa anastomosis, with the aim of simplifying the complicated steps of the conventional BA (c-BA). Thus, we observe if a difference in the risk of postoperative pancreatic fistula (POPF) exists between the two methods.
Methods: The m-BA anastomosis method has been used since 2010. From October 2011 to October 2015, 147 patients who underwent pancreatoduodenectomy (PD) using BA in Tianjin Medical University Cancer Institute and Hospital were enrolled in this study. According to the type of pancreatojejunostomy (PJ), 50 patients underwent m-BA and 97 received c-BA. The two patient cohorts were compared prospectively to some extent but not randomized, and the evaluated variables were operation time, the incidence rate of POPF, and other perioperative complications.
Results: The operation time showed no significant difference (P > 0.05) between the two groups, but the time of duct-to-mucosa anastomosis in the m-BA group was much shorter than that in the c-BA group ( P < 0.001). The incidence rate of clinically relevant POPF was 12.0% (6/50) in the modified group and 10.3% (10/97) in the conventional group ( P > 0.05), which means that the modified anastomosis method did not cause additional pancreatic leakage. The mean length of postoperative hospital stay of the m-BA group was 23 days, and that of the c-BA group was 22 days ( P > 0.05).
Conclusions: Compared with the conventional BA, we suggest that the modified BA is a feasible, safe, and effective operation method for P J of PD with no sacrifice of surgical quality. In the multivariate analysis, we also found that body mass index (≥ 25 kg/m2) increased the risk of POPF.
Keywords: Pancreatoduodenectomy; modified Blumgart anastomosis; pancreatojejunostomy; postoperative complications; postoperative pancreatic fistula.
Figures
References
-
- Aranha GV, Hodul PJ, Creech S, Jacobs W. Zero mortality after 152 consecutive pancreaticoduodenectomies with pancreaticogastrostomy. J Am Coll Surg. 2003;197:223–32. - PubMed
-
- Kleespies A, Rentsch M, Seeliger H, Albertsmeier M, Jauch K W, Bruns C J. Blumgart anastomosis for pancreaticojejunostomy minimizes severe complications after pancreatic head resection. Br J Surg. 2009;96:741–50. - PubMed
-
- Grobmyer SR, Pieracci FM, Allen PJ, Brennan MF, Jaques DP. Defining morbidity after pancreaticoduodenectomy: use of a prospective complication grading system. J Am Coll Surg. 2007;204:356–64. - PubMed
-
- Fujii T, Sugimoto H, Yamada S, Kanda M, Suenaga M, Takami H, et al. Modified blumgart anastomosis for pancreaticojejunostomy: technical improvement in matched historical control study. J Gastrointest Surg. 2014;18:1108–15. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources