

The Xomed Monopolar Cranial Nerve Stimulator Electrode: A Surprising Handy Tool for Deep Dissection of Epidermoid Tumors
- PMID: 29545981
- PMCID: PMC5849351
- DOI: 10.7759/cureus.2058
The Xomed Monopolar Cranial Nerve Stimulator Electrode: A Surprising Handy Tool for Deep Dissection of Epidermoid Tumors
Abstract
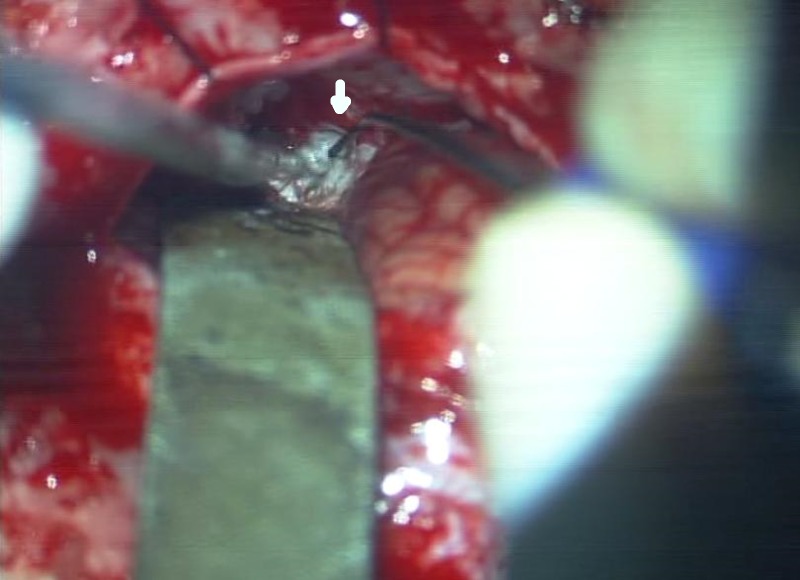
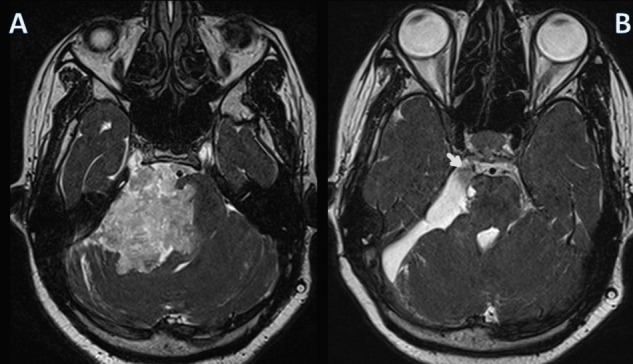
Epidermoid cysts are notorious for their propensity to sneak into deep recesses between cranial nerves in the posterior fossa. Attempts to achieve complete excision using ordinary instruments when tempted by the seeming ease of dissection is known to cause unacceptable deficits. The Xomed monopolar stimulator electrode probe of the nerve integrity electromyography monitor has several advantages when used as the primary dissection tool for deep-seated epidermoid cysts. Cerebellopontine angle epidermoid is the classical prototype of a strategically placed deep-seated epidermoid tumor. The author describes the use of the monopolar stimulator electrode of the nerve integrity electromyography monitor as the primary dissection tool for excising epidermoid cysts of the cerebellopontine angle. Thin profile, rounded nontraumatic tip, and springiness of the body of the monopolar electrode aid the dissection. The monopolar electrode was used to tease and scoop out the flakes aided by a fine suction. An initial internal decompression allowed the capsule to be folded away and separated from neurovascular structures using the dissector. The thin profile of both the instruments allowed good visualization and delicate control over the dissection in depths of the resection cavity without undue traction or impacts on superficially dissected cranial nerves. This novel use of the monopolar electrode was employed in the surgical excision of epidermoid cysts of the cerebellopontine angle in nine patients. Total or near total excision was possible in eight of the nine patients who underwent excision using this technique. In three patients, mild deficits primarily of the fifth nerve sensory function were noted. The Xomed monopolar stimulating electrode of the nerve integrity electromyography monitor is an ideal instrument for deep dissection of epidermoid cysts in areas where neurovascular structures are at risk.
Keywords: cerebellopontine angle; cranial nerve palsy; electromyography; epidermoid cyst; iatrogenic injury; intraoperative neuromonitoring; intraoperative physiological monitoring.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
The combined microscopic-endoscopic technique for radical resection of cerebellopontine angle tumors.J Neurosurg. 2015 Nov;123(5):1301-11. doi: 10.3171/2014.10.JNS141465. Epub 2015 Apr 24. J Neurosurg. 2015. PMID: 25909571
-
Cerebellopontine angle epidermoid cysts: clinical presentations and surgical outcome.Neurosurg Rev. 2016 Apr;39(2):259-66; discussion 266-7. doi: 10.1007/s10143-015-0684-5. Epub 2015 Nov 14. Neurosurg Rev. 2016. PMID: 26566990
-
Retrosigmoid Craniotomy for Resection of an Epidermoid Cyst of the Posterior Fossa.J Neurol Surg B Skull Base. 2018 Dec;79(Suppl 5):S411-S412. doi: 10.1055/s-0038-1669980. Epub 2018 Sep 25. J Neurol Surg B Skull Base. 2018. PMID: 30456045 Free PMC article.
-
Brainstem epidermoid cyst: An update.Asian J Neurosurg. 2016 Jul-Sep;11(3):194-200. doi: 10.4103/1793-5482.145163. Asian J Neurosurg. 2016. PMID: 27366244 Free PMC article. Review.
-
Cerebellopontine angle epidermoids presenting with cranial nerve hyperactive dysfunction: pathogenesis and long-term surgical results in 30 patients.Neurosurgery. 2002 Feb;50(2):276-85; discussion 285-6. doi: 10.1097/00006123-200202000-00008. Neurosurgery. 2002. PMID: 11844262 Review.
References
-
- Surgery of intracranial epidermoid cysts. Report of 44 patients and review of the literature. [Article in French] Lopes M, Capelle L, Duffau H, et al. https://www.ncbi.nlm.nih.gov/pubmed/11972145. Neurochirurgie. 2002;48:5–13. - PubMed
-
- Surgical treatment of epidermoid cysts of the cerebellopontine angle. Samii M, Tatagiba M, Piquer J, Carvalho GA. http://10.3171/jns.1996.84.1.0014. J Neurosurg. 1996;84:14–19. - PubMed
-
- Experience with cerebellopontine angle epidermoids. Mohanty A, Venkatrama SK, Rao BR, Chandramouli BA, Jayakumar PN, Das BS. https://www.ncbi.nlm.nih.gov/pubmed/8971820. Neurosurgery. 1997;40:24–29. - PubMed
-
- Epidermoids of the cerebellopontine angle: a 20-year experience. Schiefer TK, Link MJ. Surg Neurol. 2008;70:584–590. - PubMed
-
- Clinical course and surgical prognosis of 33 cases of intracranial epidermoid tumors. Yamakawa K, Shitara N, Genka S, Manaka S, Takakura K. https://www.ncbi.nlm.nih.gov/pubmed/2710302. Neurosurgery. 1989;24:568–573. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources