

Virus-Specific Antibody, Viral Load, and Disease Severity in Respiratory Syncytial Virus Infection
- PMID: 29546402
- PMCID: PMC6009588
- DOI: 10.1093/infdis/jiy106
Virus-Specific Antibody, Viral Load, and Disease Severity in Respiratory Syncytial Virus Infection
Abstract
Background: Maternally derived serum antibody and viral load are thought to influence disease severity in primary respiratory syncytial virus (RSV) infection. As part of the AsPIRES study of RSV pathogenesis, we correlated various serum antibody concentrations and viral load with disease severity.
Methods: Serum neutralizing antibody titers and levels of immunoglobulin G (IgG) to RSV fusion protein (F), attachment proteins of RSV group A and B, the CX3C region of G, and nasal viral load were measured in 139 full-term previously healthy infants with primary RSV infection and correlated with illness severity.
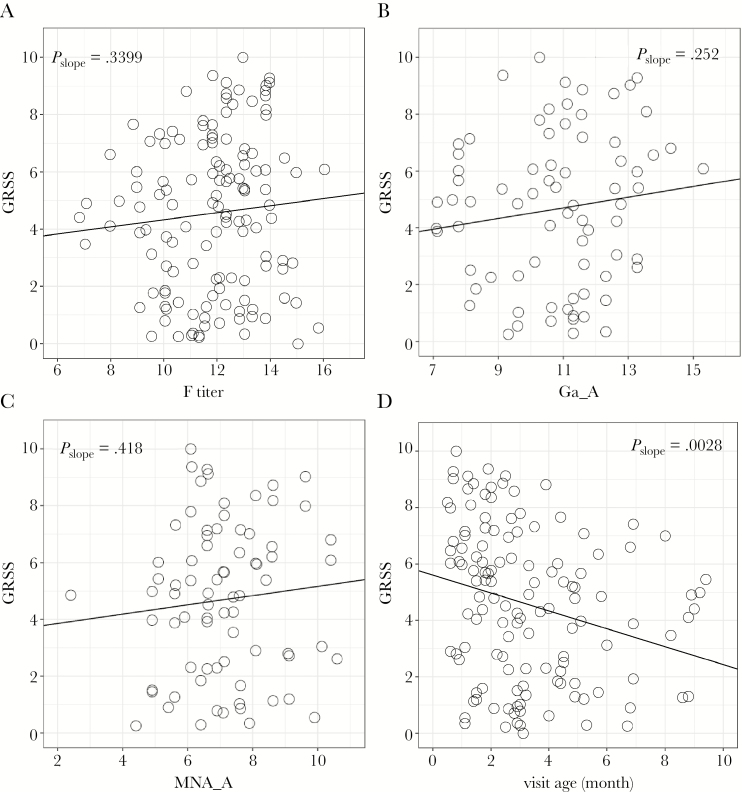
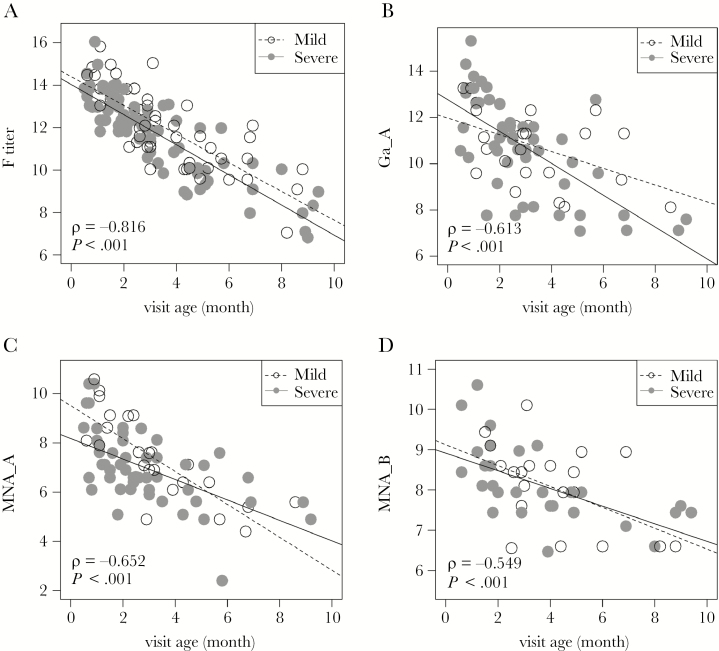
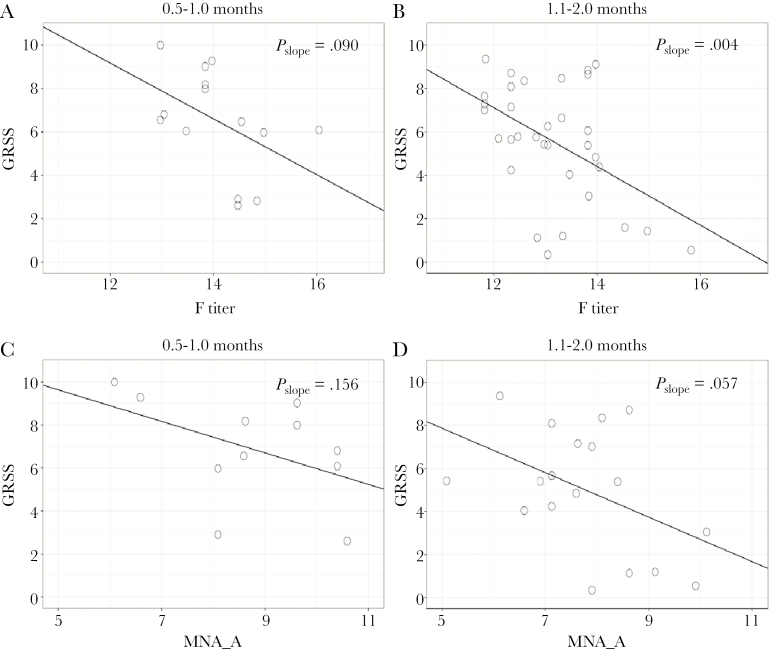
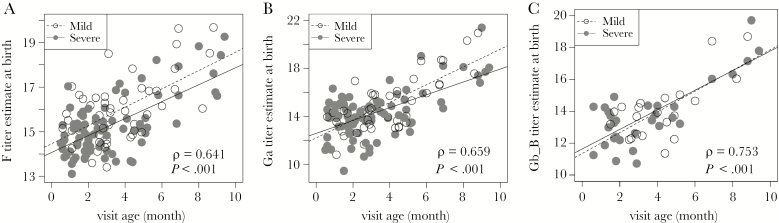
Results: Univariate analysis showed no relationship between measures of serum antibody and severity. However, a multivariate model adjusting for age at the time of infection found a significant 0.56 decrease in severity score for each 2-fold increase in antibody concentration to RSV F. The benefit of antibody was greatest in infants ≤ 2 months of age. Additionally, estimated antibody titer at birth was correlated with age at infection, suggesting that higher antibody titers delay infection. Viral load did not differ by illness severity.
Conclusion: Our data support the concept of maternal immunization with an RSV vaccine during pregnancy as a strategy for reducing the burden of RSV infection in full-term healthy infants exposed to RSV during their first winter.
Figures
References
-
- Hall CB, Weinberg GA, Blumkin AK et al. . Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics 2013; 132:e341–8. - PubMed
-
- Meissner HC. Viral bronchiolitis in children. N Engl J Med 2016; 374:62–72. - PubMed
-
- Glezen WP, Paredes A, Allison JE, Taber LH, Frank AL. Risk of respiratory syncytial virus infection for infants from low-income families in relationship to age, sex, ethnic group, and maternal antibody level. J Pediatr 1981; 98:708–15. - PubMed
-
- Holberg CJ, Wright AL, Martinez FD, Ray CG, Taussig LM, Lebowitz MD. Risk factors for respiratory syncytial virus-associated lower respiratory illnesses in the first year of life. Am J Epidemiol 1991; 133:1135–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
