

A national evaluation of the management practices of hemorrhoidal disease in the Netherlands
- PMID: 29546558
- PMCID: PMC5899108
- DOI: 10.1007/s00384-018-3019-5
A national evaluation of the management practices of hemorrhoidal disease in the Netherlands
Abstract
Purpose: In this study, we describe current practices in the management of hemorrhoidal disease in the Netherlands.
Methods: A validated online survey was performed among Dutch surgeons and residents treating hemorrhoidal disease. Contact details were retrieved from the Dutch Association for Surgery resulting in 619 contacts. Only doctors who were treating hemorrhoidal disease regularly were asked to complete the questionnaire. The following items were assessed: initial treatment, recurrence, complications, and follow-up.
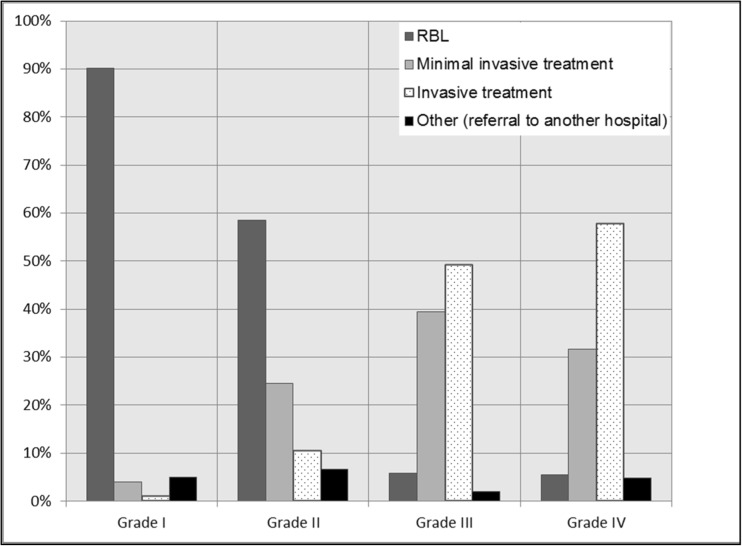
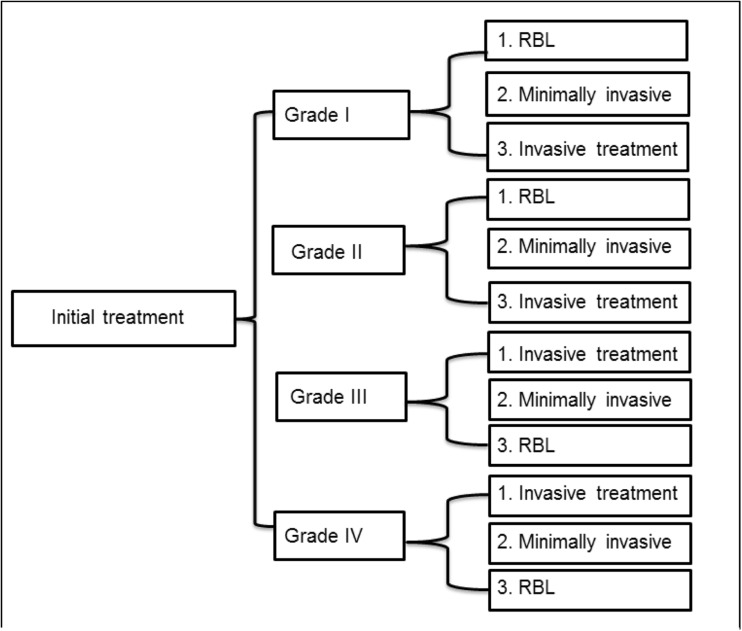
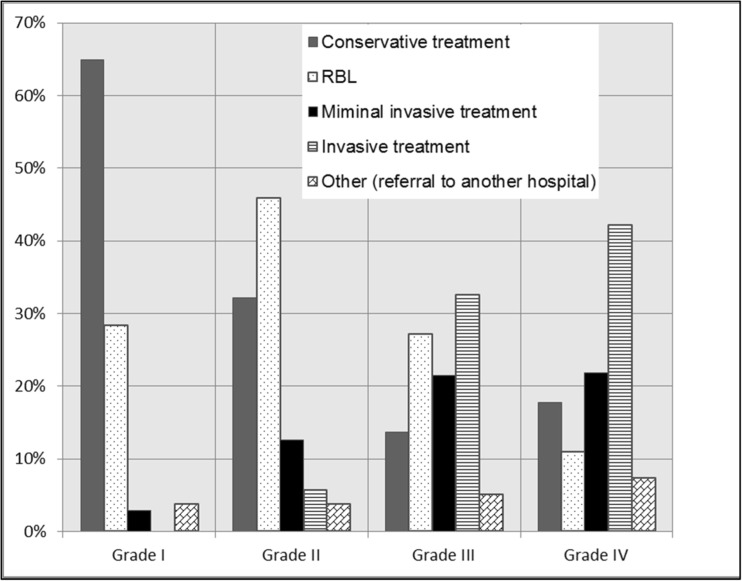
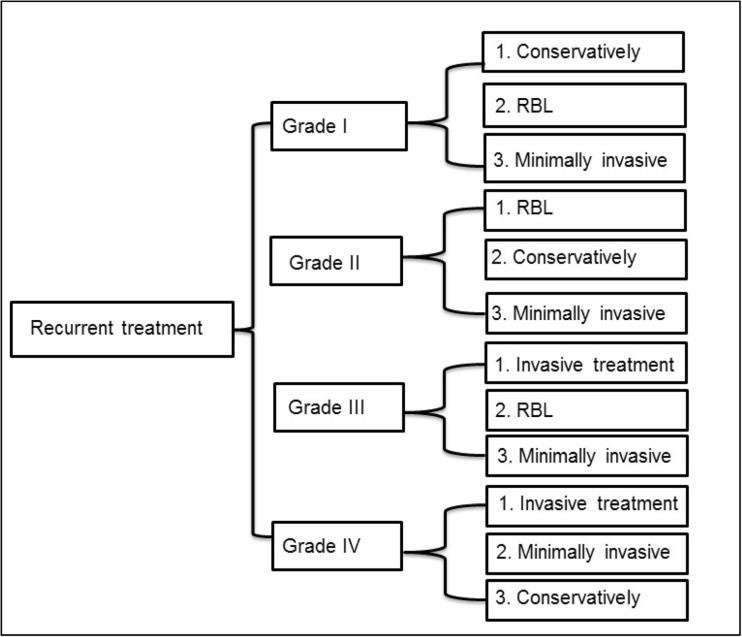
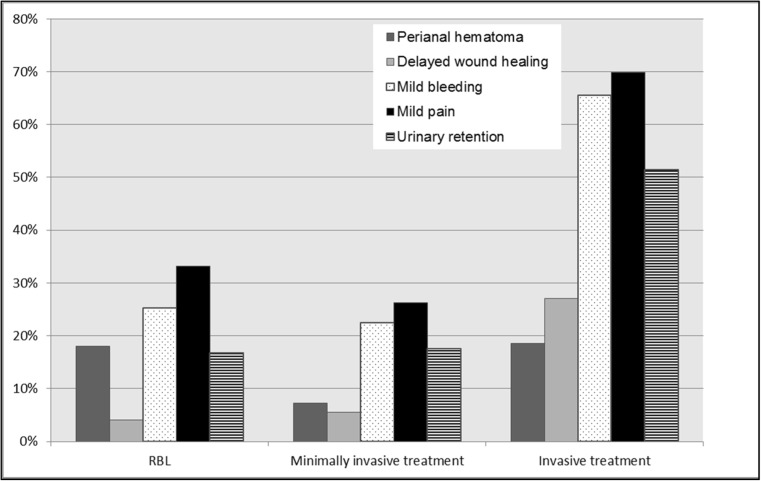
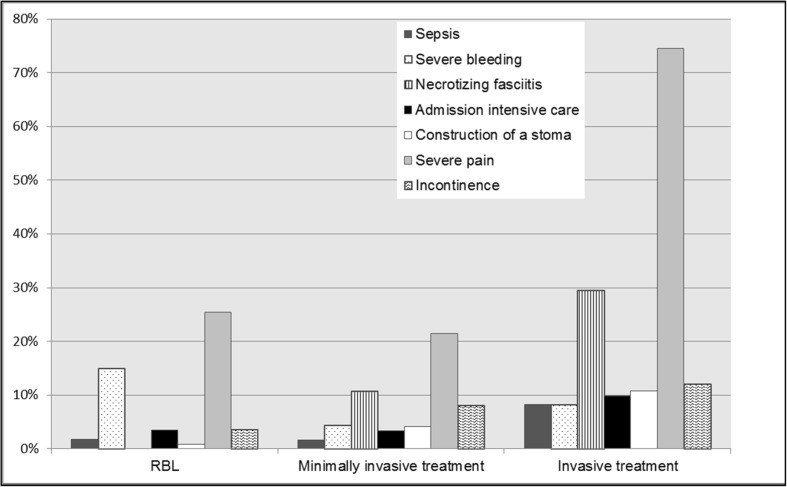
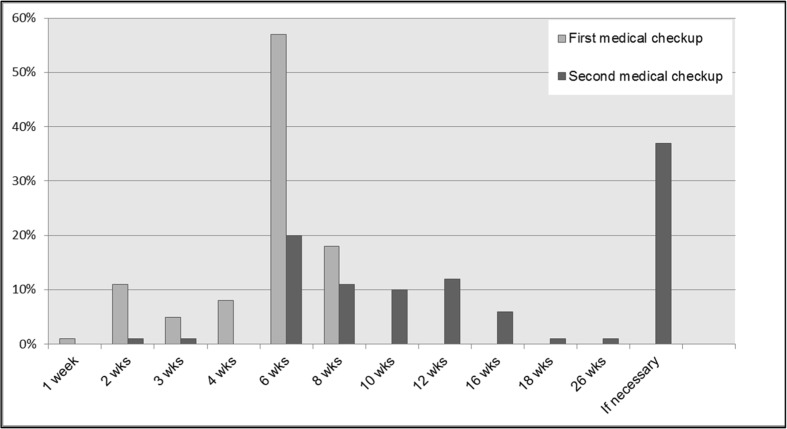
Results: In total, 133 respondents completed the survey. Ninety percent of the respondents started with rubber band ligation (RBL) as the first treatment in low-grade hemorrhoidal disease. In case of recurrence, 64% of the respondents repeated RBL three times before switching to a more invasive treatment modality. In grade III hemorrhoidal disease, the respondents preferred more invasive techniques: a sutured hemorrhoidopexy was performed in 24%, Doppler-guided hemorrhoidal artery ligation (DG-HAL) in 9%, stapled hemorrhoidopexy in 19%, and the traditional hemorrhoidectomy in 31% of the patients, respectively. The majority of the respondents (39%) reported a mild complication in 5-10% of the patients. The most reported complication was pain. Nearly all the respondents (98%) reported a major complication in less than 5% of the patients. The majority of the patients (57%) were seen in outpatient clinics 6 weeks post-treatment.
Conclusion: This Dutch survey showed areas of common practice for primary treatment of hemorrhoidal disease. However, it also demonstrated varying practices regarding recurrent hemorrhoidal disease. Practical guidelines are required to support colorectal surgeons in the Netherlands.
Keywords: Hemorrhoids; Surgical; Survey; Therapy; Treatment algorithm.
Conflict of interest statement
The ethical committee of Maastricht University Medical Centre confirmed that the Medical Research Involving Human Subjects Act (WMO) does not apply to the abovementioned study and that an official approval of this study by the committee is not required.
Figures
References
-
- Russell, MMG, Ko CY (2012) Management of hemorrhoids: mainstay of treatment remains diet modification and office-based procedures July 16, 2012
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
