

Partners and Alerts in Medication Adherence: A Randomized Clinical Trial
- PMID: 29546659
- PMCID: PMC6109000
- DOI: 10.1007/s11606-018-4389-7
Partners and Alerts in Medication Adherence: A Randomized Clinical Trial
Abstract
Background: Poor medication adherence is common and limits the effectiveness of treatment.
Objective: To investigate how social supports, automated alerts, and their combination improve medication adherence.
Design: Four-arm, randomized clinical trial with a 6-month intervention.
Participants: A total of 179 CVS health employees or adult dependents with CVS Caremark prescription coverage, a current daily statin prescription, a medication possession ratio less than 80%, and Internet access.
Interventions: Participants were randomly assigned to control, social support (partner), automated adherence alert messages (alert), or both social support and alerts (partner + alert). Participants in the social support arms were asked to name a medication adherence partner (MAP) to help them take their medication. Participants in the alert arms were sent emails, text messages, or automated phone calls if they had failed to adhere on the previous day and on one or both of the 2 days before that. In partner + alert, both participants and fully enrolled MAPs received alerts.
Main measures: Adherence measured by wireless pill bottle opening.
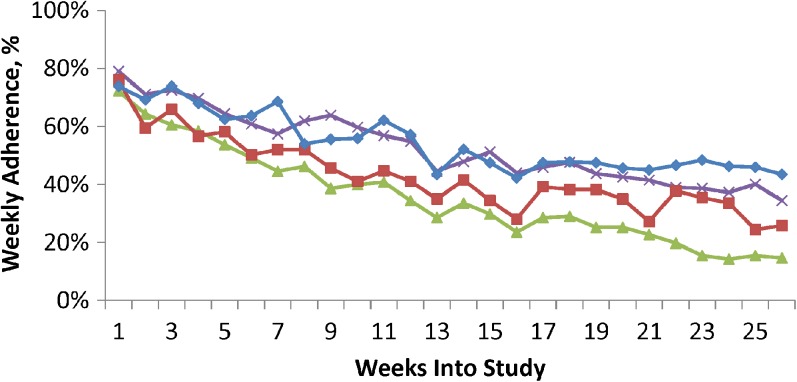
Key results: Compared to 36.0% adherence in control, adherence was significantly greater in the alert arm (52.9%, difference vs. control of 17.0%, 95% CI for difference 6.3 to 27.6%, P = 0.002) and the partner + alert arm (54.5%, difference vs. control of 18.6%, 95% CI for difference 6.6 to 30.5%, P = 0.003). Adherence in the partner arm was not statistically significantly greater than control (43.2%, difference vs. control of 7.2%, 95% CI of difference - 5.2% to 19.5%, P = 0.25). There were no statistically significant differences among the three treatment arms. Fewer participants invited a MAP in the partner + alert arm than the partner arm (P = 0.02).
Conclusions: Automated alerts were effective at improving medication adherence. Assigning a medication adherence partner did not statistically significantly affect adherence rates.
Trial registration: ClinicalTrials.gov Number NCT01890018 [ https://clinicaltrials.gov /].
Keywords: medication adherence; medication alerts; support partner.
Conflict of interest statement
Compliance with ethical standards
The study was approved by the Institutional Review Board of the University of Pennsylvania and registered on
Conflict of Interest
All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Drs. Asch and Volpp are principals at the behavioral economics consulting firm VAL Health. Dr. Troxel serves on the scientific advisory board of VAL Health. Dr. Volpp has received consulting income from CVS Caremark and research funding from Humana, CVS Caremark, Discovery/Vitality (South Africa insurer and health incentives company, not the manufacturer of Vitality Glowcaps), Hawaii Medical Services Association, Weight Watchers, and Merck. Dr. Shrank is employed and salaried by UPMC Health Plan. Dr. Brennan is employed and salaried by CVS Health Corporation. All other authors declare no conflicts of interest.
Presentation
AcademyHealth Annual Research Meeting, June 28, 2016.
Figures

References
-
- Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383–9 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
