

No differences in objective dynamic instability during acceleration of the knee with or without subjective instability post-total knee arthroplasty
- PMID: 29547641
- PMCID: PMC5856396
- DOI: 10.1371/journal.pone.0194221
No differences in objective dynamic instability during acceleration of the knee with or without subjective instability post-total knee arthroplasty
Abstract
Introduction: Instability after total knee arthroplasty is a critical problem. The purpose of this study was to clarify the stability of implanted knees during walking by comparing differences in dynamic instability during knee acceleration between individuals with or without previously experienced subjective instability, as measured by self-reported questionnaire.
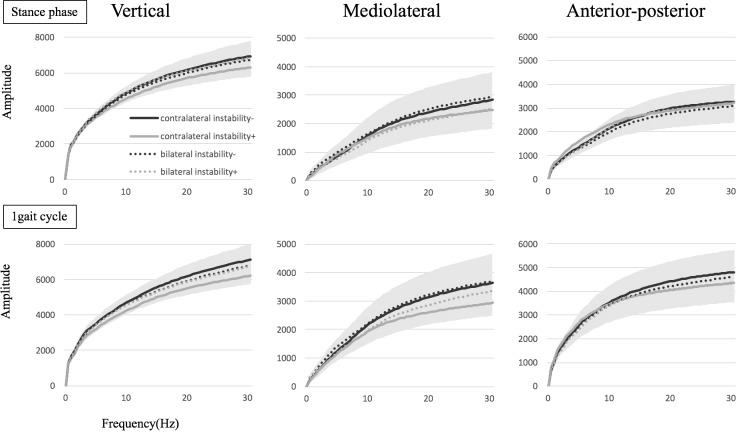
Materials and methods: We examined 92 knees with medial pivot implants. Mean patient age and follow-up duration were 78.4 years and 32.8 months, respectively. An accelerometer was used to investigate the accelerations along three axes; that is, vertical (VT), mediolateral (ML), and anteroposterior (AP) directions in 3-dimensional (3D) space. The analysis in the stance phase and gait cycle was performed by: (1) root mean square (RMS) values of acceleration and (2) frequency domain analysis using fast Fourier transformation (FFT). A self-reported knee instability score was used for the subjective feeling of instability.
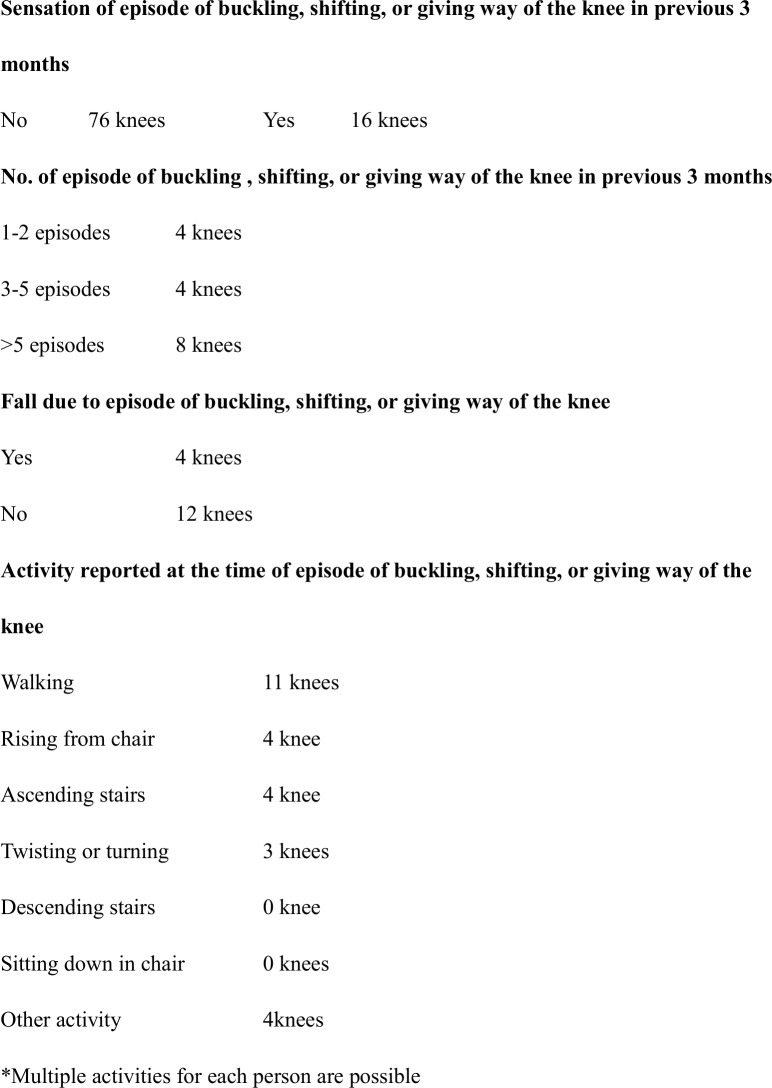
Results: A total of 76 knees did not feel unstable (group 0), but 16 knees felt unstable (group 1) in patients during activities of daily living. Regarding the RMS, there were no differences in each direction between the groups. For FFT, the cumulative amplitude in the frequency < 30 Hz also showed no significant differences in all directions between the groups during the stance phase (VT, p = 0.335; ML, p = 0.219; AP, p = 0.523) or gait cycle (VT, p = 0.077; ML, p = 0.082; AP, p = 0.499).
Discussion: Gait analysis based on the acceleration data showed that there were no between-group differences in objective dynamic instability during acceleration of the knee, with or without reports of previously experienced subjective instability, as assessed by the self-reported questionnaire.
Conflict of interest statement
Figures



Similar articles
-
Association between anteroposterior laxity in mid-range flexion and subjective healing of instability after total knee arthroplasty.Knee Surg Sports Traumatol Arthrosc. 2017 Nov;25(11):3543-3548. doi: 10.1007/s00167-016-4375-8. Epub 2016 Nov 9. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 27830283
-
Acceleration-based joint stability parameters for total knee arthroplasty that correspond with patient-reported instability.Proc Inst Mech Eng H. 2013 Oct;227(10):1104-13. doi: 10.1177/0954411913493724. Epub 2013 Jul 25. Proc Inst Mech Eng H. 2013. PMID: 23886970 Clinical Trial.
-
Anterior translation and rotational stability of anterior cruciate ligament-deficient knees during walking: speed and turning direction.J Orthop Sci. 2015 Jan;20(1):155-62. doi: 10.1007/s00776-014-0672-6. Epub 2014 Nov 14. J Orthop Sci. 2015. PMID: 25395272
-
Association of a Wider Medial Gap (Medial Laxity) in Flexion with Self-Reported Knee Instability After Medial-Pivot Total Knee Arthroplasty.J Bone Joint Surg Am. 2022 May 18;104(10):910-918. doi: 10.2106/JBJS.21.01034. Epub 2022 Mar 23. J Bone Joint Surg Am. 2022. PMID: 35320136
-
The unstable knee: wobble and buckle.Bone Joint J. 2014 Nov;96-B(11 Supple A):112-4. doi: 10.1302/0301-620X.96B11.34325. Bone Joint J. 2014. PMID: 25381421 Review.
Cited by
-
Inter-Rater Reliability of Clinical Testing for Laxity After Knee Arthroplasty.J Arthroplasty. 2022 Jul;37(7):1296-1301. doi: 10.1016/j.arth.2022.03.044. Epub 2022 Mar 17. J Arthroplasty. 2022. PMID: 35307526 Free PMC article.
-
Correlation of quality of life with instrumented analysis of a total knee arthroplasty series at the long-term follow-up.Eur J Orthop Surg Traumatol. 2021 Aug;31(6):1171-1177. doi: 10.1007/s00590-020-02867-0. Epub 2021 Jan 8. Eur J Orthop Surg Traumatol. 2021. PMID: 33417050
-
Wearable sensor systems measure differences in knee laxity between healthy and affected knees during dynamic exercise activities: A systematic review.J Exp Orthop. 2024 Jul 24;11(3):e12094. doi: 10.1002/jeo2.12094. eCollection 2024 Jul. J Exp Orthop. 2024. PMID: 39055395 Free PMC article. Review.
-
Current clinical utilisation of wearable motion sensors for the assessment of outcome following knee arthroplasty: a scoping review.BMJ Open. 2019 Dec 29;9(12):e033832. doi: 10.1136/bmjopen-2019-033832. BMJ Open. 2019. PMID: 31888943 Free PMC article.
-
The assessment of instability in the osteoarthritic knee.EFORT Open Rev. 2019 Mar 8;4(3):70-76. doi: 10.1302/2058-5241.4.170079. eCollection 2019 Mar. EFORT Open Rev. 2019. PMID: 30993008 Free PMC article. Review.
References
-
- Colizza WA, Insall JN, Scuderi GR. The posterior-stabilized knee prosthesis: assessment of polyethylene damage and osteolysis after a ten-year minimum follow-up. J Bone Joint Surg Am. 1995;77:1713–20. - PubMed
-
- Emmerson KP, Moran CG, Pinder IM. Survivorship analysis of the kinematic stabilizer total knee replacement: a 10–14 year follow-up. J Bone Joint Surg Br. 1996;78:441–5. - PubMed
-
- Fort-Rodriquez DE, Scuderi GR, Insall JN. Survivorship of cemented total knee arthroplasty. Clin Orthop Relat Res. 1997;345:79–86. - PubMed
-
- Pagnano MW, Hanssen AD, Lewallen DG, Stuart ML. Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop Relat Res. 1998;356:39–46. - PubMed
-
- Mochizuki T, Tanifuji O, Sato T, Hijikata H, Koga H, Watanabe S, et al. Association between anteroposterior laxity in mid-range flexion and subjective healing of instability after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2017;25:3543–8. doi: 10.1007/s00167-016-4375-8 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
