

Effect of Seasonal Variation on Clinical Outcome in Patients with Chronic Conditions: Analysis of the Commonwealth Scientific and Industrial Research Organization (CSIRO) National Telehealth Trial
- PMID: 29549068
- PMCID: PMC5878365
- DOI: 10.2196/medinform.9680
Effect of Seasonal Variation on Clinical Outcome in Patients with Chronic Conditions: Analysis of the Commonwealth Scientific and Industrial Research Organization (CSIRO) National Telehealth Trial
Abstract
Background: Seasonal variation has an impact on the hospitalization rate of patients with a range of cardiovascular diseases, including myocardial infarction and angina. This paper presents findings on the influence of seasonal variation on the results of a recently completed national trial of home telemonitoring of patients with chronic conditions, carried out at five locations along the east coast of Australia.
Objective: The aim is to evaluate the effect of the seasonal timing of hospital admission and length of stay on clinical outcome of a home telemonitoring trial involving patients (age: mean 72.2, SD 9.4 years) with chronic conditions (chronic obstructive pulmonary disease coronary artery disease, hypertensive diseases, congestive heart failure, diabetes, or asthma) and to explore methods of minimizing the influence of seasonal variations in the analysis of the effect of at-home telemonitoring on the number of hospital admissions and length of stay (LOS).
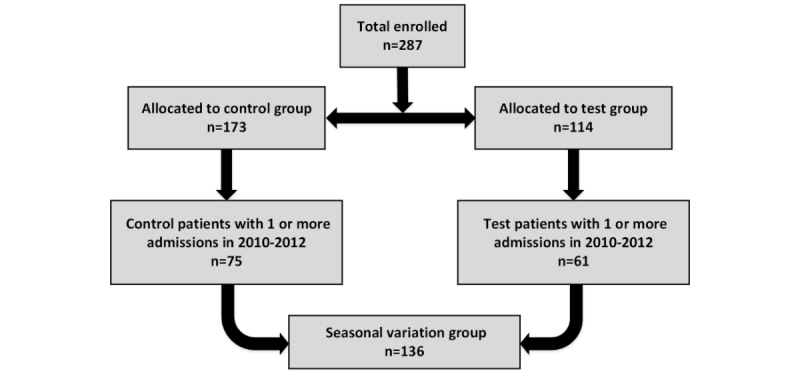
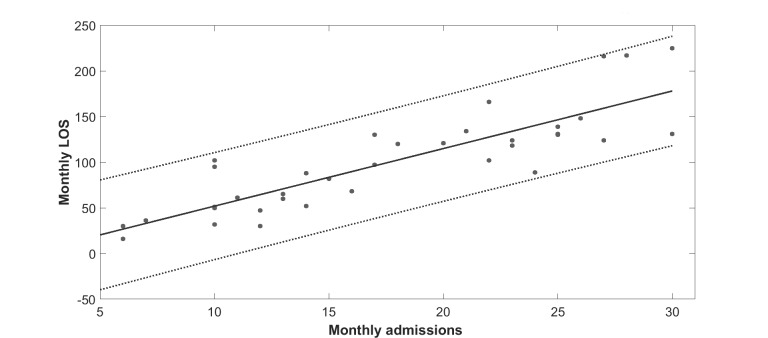
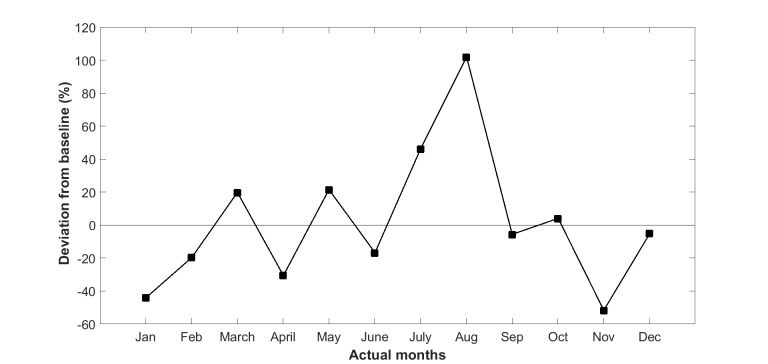
Methods: Patients were selected from a hospital list of eligible patients living with a range of chronic conditions. Each test patient was case matched with at least one control patient. A total of 114 test patients and 173 control patients were available in this trial. However, of the 287 patients, we only considered patients who had one or more admissions in the years from 2010 to 2012. Three different groups were analyzed separately because of substantially different climates: (1) Queensland, (2) Australian Capital Territory and Victoria, and (3) Tasmania. Time series data were analyzed using linear regression for a period of 3 years before the intervention to obtain an average seasonal variation pattern. A novel method that can reduce the impact of seasonal variation on the rate of hospitalization and LOS was used in the analysis of the outcome variables of the at-home telemonitoring trial.
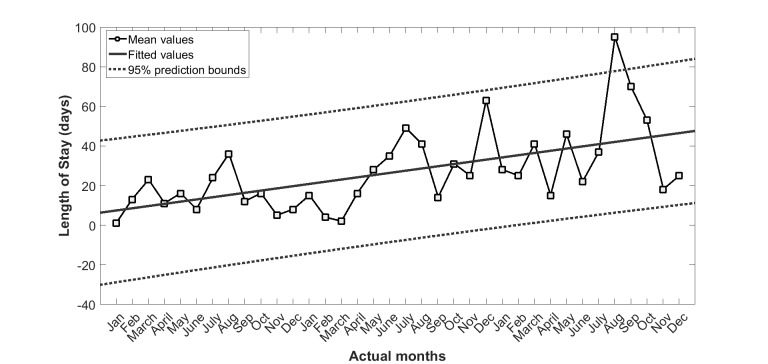
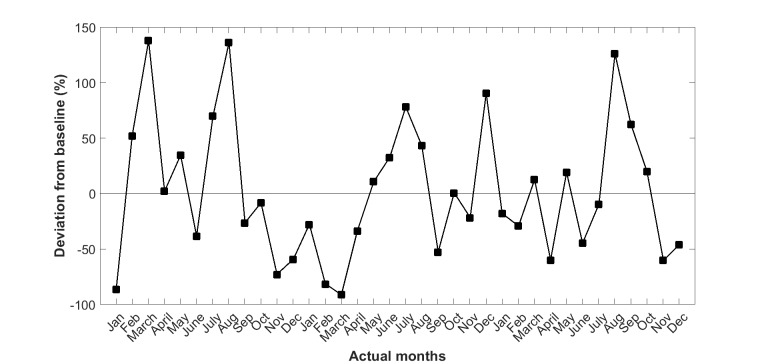
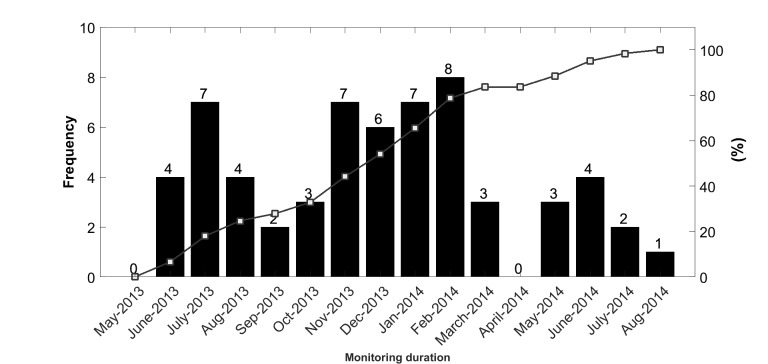
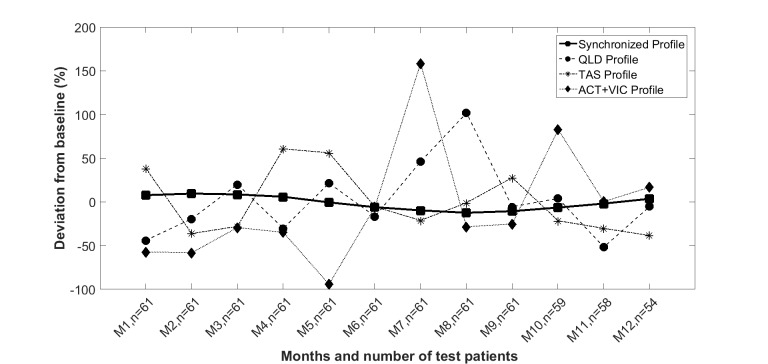
Results: Test patients were monitored for a mean 481 (SD 77) days with 87% (53/61) of patients monitored for more than 12 months. Trends in seasonal variations were obtained from 3 years' of hospitalization data before intervention for the Queensland, Tasmania, and Australian Capital Territory and Victoria subgroups, respectively. The maximum deviation from baseline trends for LOS was 101.7% (SD 42.2%), 60.6% (SD 36.4%), and 158.3% (SD 68.1%). However, by synchronizing outcomes to the start date of intervention, the impact of seasonal variations was minimized to a maximum of 9.5% (SD 7.7%), thus improving the accuracy of the clinical outcomes reported.
Conclusions: Seasonal variations have a significant effect on the rate of hospital admission and LOS in patients with chronic conditions. However, the impact of seasonal variation on clinical outcomes (rate of admissions, number of hospital admissions, and LOS) of at-home telemonitoring can be attenuated by synchronizing the analysis of outcomes to the commencement dates for the telemonitoring of vital signs.
Trial registration: Australian New Zealand Clinical Trial Registry ACTRN12613000635763; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=364030&isReview=true (Archived by WebCite at http://www.webcitation.org/ 6xLPv9QDb).
Keywords: chronic disease; clinical trial; seasonal variation; telehealth; telemonitoring; vital signs.
©Ahmadreza Argha, Andrey Savkin, Siaw-Teng Liaw, Branko George Celler. Originally published in JMIR Medical Informatics (http://medinform.jmir.org), 16.03.2018.
Conflict of interest statement
Conflicts of Interest: There was no conflict of interest during the planning and execution of the project. Six months after its completion, BGC, Chief Investigator and Project Director, was appointed to a part-time position at Telemedcare Pty Ltd as Director of Research.
Figures

Similar articles
-
Patient Adherence to Scheduled Vital Sign Measurements During Home Telemonitoring: Analysis of the Intervention Arm in a Before and After Trial.JMIR Med Inform. 2018 Apr 9;6(2):e15. doi: 10.2196/medinform.9200. JMIR Med Inform. 2018. PMID: 29631991 Free PMC article.
-
Impact of At-Home Telemonitoring on Health Services Expenditure and Hospital Admissions in Patients With Chronic Conditions: Before and After Control Intervention Analysis.JMIR Med Inform. 2017 Sep 8;5(3):e29. doi: 10.2196/medinform.7308. JMIR Med Inform. 2017. PMID: 28887294 Free PMC article.
-
Seasonal Variation In An At-Home Telemonitoring Trial.Annu Int Conf IEEE Eng Med Biol Soc. 2018 Jul;2018:1-4. doi: 10.1109/EMBC.2018.8512495. Annu Int Conf IEEE Eng Med Biol Soc. 2018. PMID: 30440255 Clinical Trial.
-
Impact of telemonitoring home care patients with heart failure or chronic lung disease from primary care on healthcare resource use (the TELBIL study randomised controlled trial).BMC Health Serv Res. 2013 Mar 28;13:118. doi: 10.1186/1472-6963-13-118. BMC Health Serv Res. 2013. PMID: 23537332 Free PMC article. Clinical Trial.
-
Effectiveness of telemonitoring versus usual care for chronic obstructive pulmonary disease: A systematic review and meta-analysis.J Telemed Telecare. 2020 May;26(4):189-199. doi: 10.1177/1357633X18811757. Epub 2018 Dec 12. J Telemed Telecare. 2020. PMID: 30541375
Cited by
-
A vital sign-based prediction algorithm for differentiating COVID-19 versus seasonal influenza in hospitalized patients.NPJ Digit Med. 2021 Jun 4;4(1):95. doi: 10.1038/s41746-021-00467-8. NPJ Digit Med. 2021. PMID: 34088961 Free PMC article.
-
Impact of Winter Season on Inpatient Outcomes and Trends in Cardiac Arrest Hospitalizations: A Nationwide Analysis.Cureus. 2025 Feb 19;17(2):e79297. doi: 10.7759/cureus.79297. eCollection 2025 Feb. Cureus. 2025. PMID: 40125174 Free PMC article.
-
Post-polio hospital admissions in Australia over a 10-year period: An observational study and analysis of trends by month, location, and comparable conditions.J Public Health (Oxf). 2025 Aug 29;47(3):e262-e273. doi: 10.1093/pubmed/fdaf029. J Public Health (Oxf). 2025. PMID: 40062475 Free PMC article.
-
Mobile phone access and preferences among medical inpatients at an urban Canadian hospital for post-discharge planning: A pre-COVID-19 cross-sectional survey.Front Digit Health. 2022 Nov 11;4:928602. doi: 10.3389/fdgth.2022.928602. eCollection 2022. Front Digit Health. 2022. PMID: 36440462 Free PMC article.
-
Digital endpoints in clinical trials: emerging themes from a multi-stakeholder Knowledge Exchange event.Trials. 2024 Aug 3;25(1):521. doi: 10.1186/s13063-024-08356-7. Trials. 2024. PMID: 39095915 Free PMC article.
References
-
- Bashshur RL, Shannon GW, Smith BR, Alverson DC, Antoniotti N, Barsan WG, Bashshur N, Brown EM, Coye MJ, Doarn CR, Ferguson S, Grigsby J, Krupinski EA, Kvedar JC, Linkous J, Merrell RC, Nesbitt T, Poropatich R, Rheuban KS, Sanders JH, Watson AR, Weinstein RS, Yellowlees P. The empirical foundations of telemedicine interventions for chronic disease management. Telemed J E Health. 2014 Sep;20(9):769–800. doi: 10.1089/tmj.2014.9981. http://europepmc.org/abstract/MED/24968105 - DOI - PMC - PubMed
-
- Bashshur RL, Howell JD, Krupinski EA, Harms KM, Bashshur N, Doarn CR. The empirical foundations of telemedicine interventions in primary care. Telemed J E Health. 2016 May;22(5):342–375. doi: 10.1089/tmj.2016.0045. http://europepmc.org/abstract/MED/27128779 - DOI - PMC - PubMed
-
- Steventon A, Bardsley M, Billings J, Dixon J, Doll H, Hirani S, Cartwright M, Rixon L, Knapp M, Henderson C, Rogers A, Fitzpatrick R, Hendy J, Newman S, Whole System Demonstrator Evaluation Team BMJ. 2012. Jun 21, [2018-02-26]. Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial https://sso.lib.uts.edu.au/cas/login?service=https%3A%2F%2Fwww.lib.uts.e... 6xWt9AoOR. - PMC - PubMed
-
- Paré G, Jaana M, Sicotte C. Systematic review of home telemonitoring for chronic diseases: the evidence base. J Am Med Inform Assoc. 2007 May;14(3):269–277. doi: 10.1197/jamia.M2270. https://sso.lib.uts.edu.au/cas/login?service=https%3A%2F%2Fwww.lib.uts.e... - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
