

Myomodulation with Injectable Fillers: An Innovative Approach to Addressing Facial Muscle Movement
- PMID: 29549406
- PMCID: PMC5945756
- DOI: 10.1007/s00266-018-1116-z
Myomodulation with Injectable Fillers: An Innovative Approach to Addressing Facial Muscle Movement
Abstract
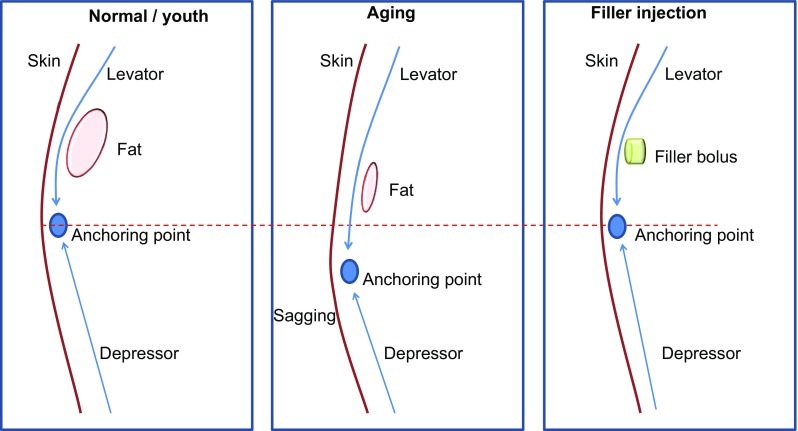
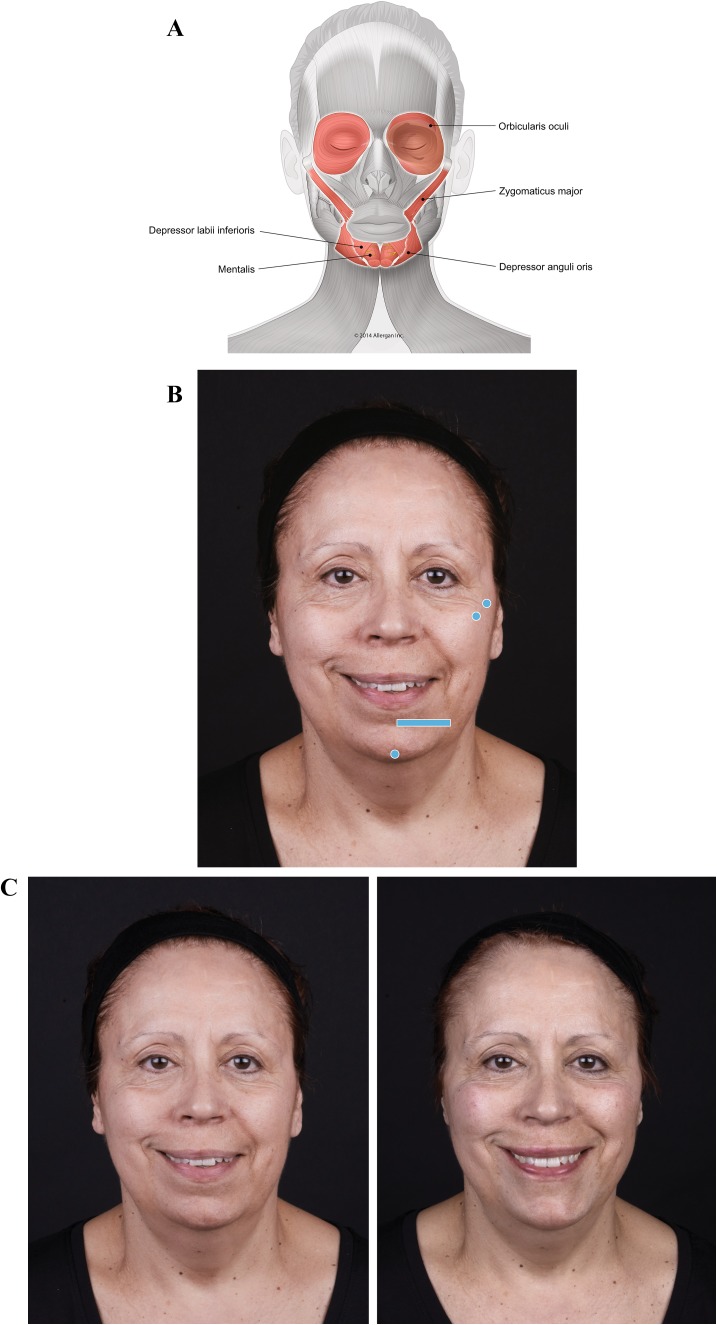
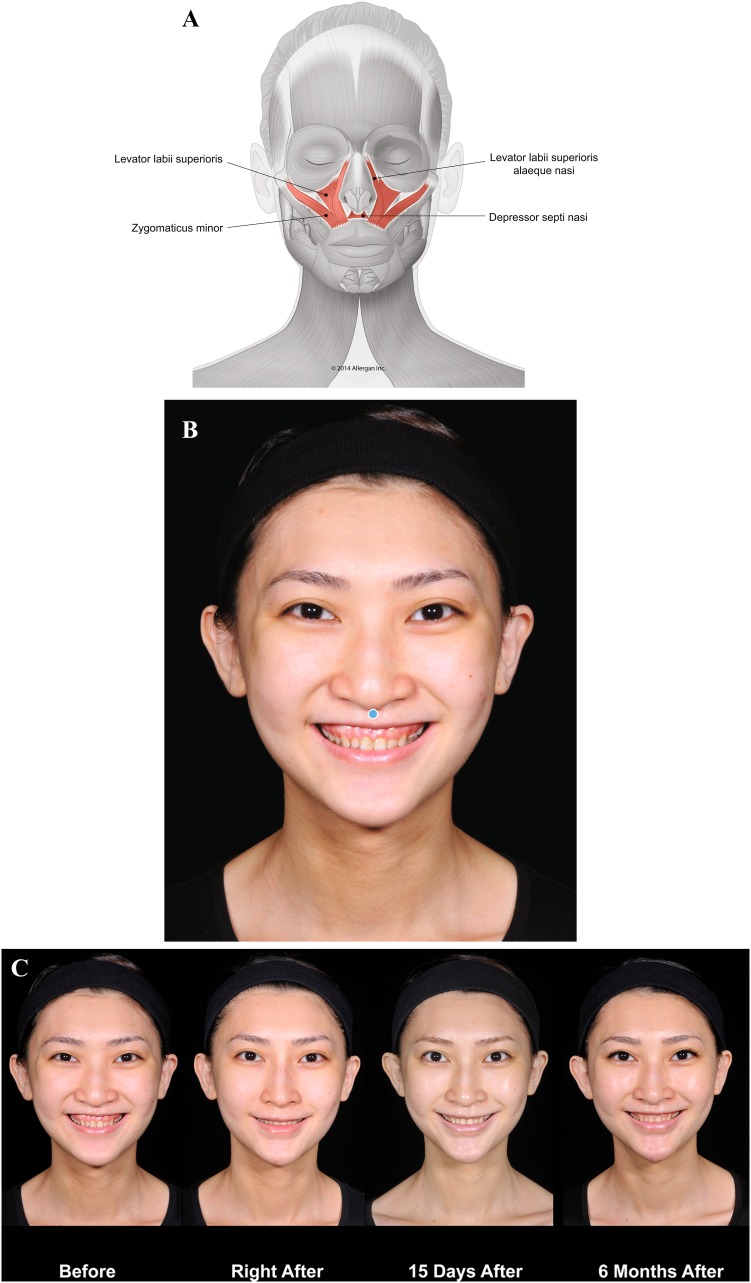
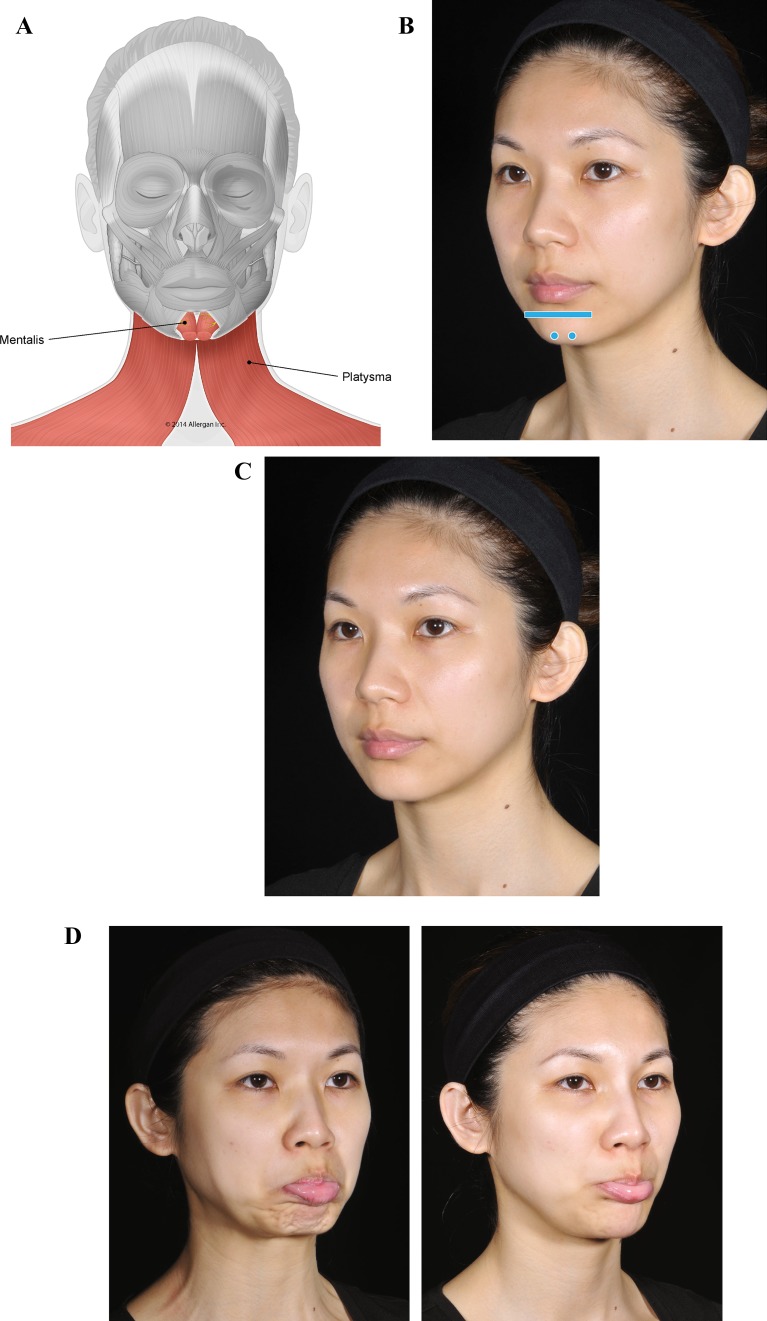
Consideration of facial muscle dynamics is underappreciated among clinicians who provide injectable filler treatment. Injectable fillers are customarily used to fill static wrinkles, folds, and localized areas of volume loss, whereas neuromodulators are used to address excessive muscle movement. However, a more comprehensive understanding of the role of muscle function in facial appearance, taking into account biomechanical concepts such as the balance of activity among synergistic and antagonistic muscle groups, is critical to restoring facial appearance to that of a typical youthful individual with facial esthetic treatments. Failure to fully understand the effects of loss of support (due to aging or congenital structural deficiency) on muscle stability and interaction can result in inadequate or inappropriate treatment, producing an unnatural appearance. This article outlines these concepts to provide an innovative framework for an understanding of the role of muscle movement on facial appearance and presents cases that illustrate how modulation of muscle movement with injectable fillers can address structural deficiencies, rebalance abnormal muscle activity, and restore facial appearance.
Level of evidence v: This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266 .
Keywords: Esthetic facial procedures; Hyaluronic acid; Injectable fillers; Myomodulation; Palsy.
Conflict of interest statement
MDM is an Allergan plc consultant for speaking events and medical education.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
