

Methods to estimate access to care and the effect of interventions on the outcomes of congenital disorders
- PMID: 29549604
- PMCID: PMC6167260
- DOI: 10.1007/s12687-018-0359-3
Methods to estimate access to care and the effect of interventions on the outcomes of congenital disorders
Abstract
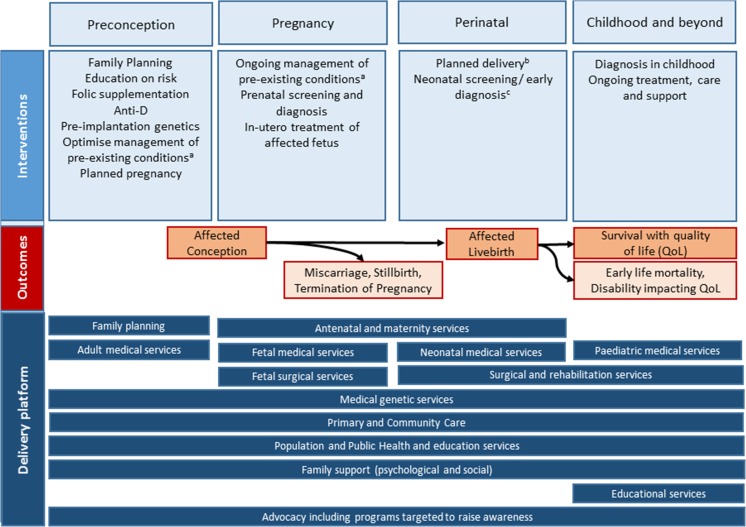
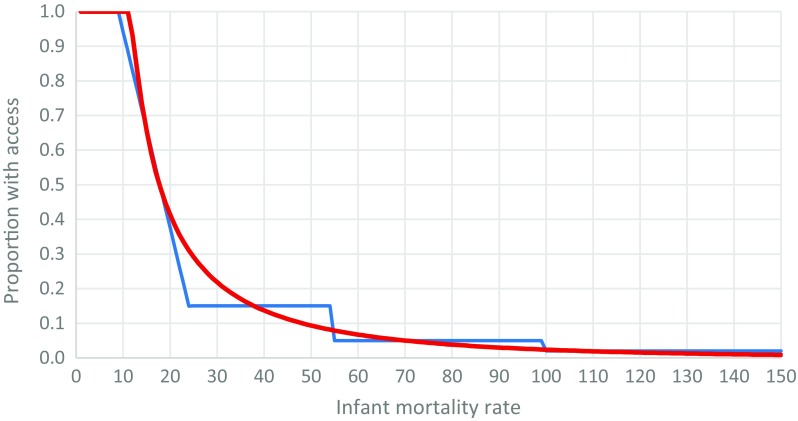
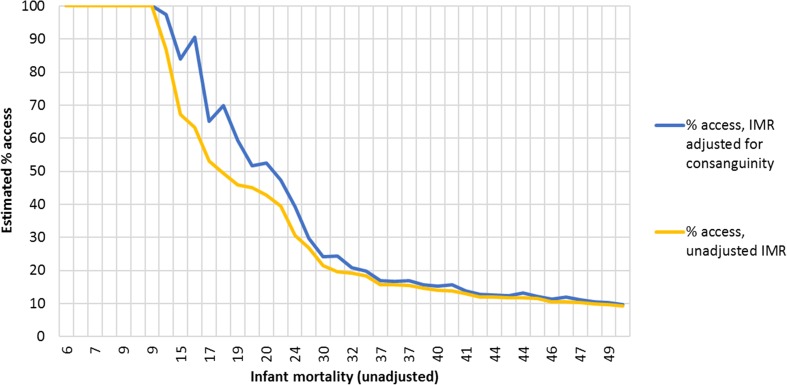
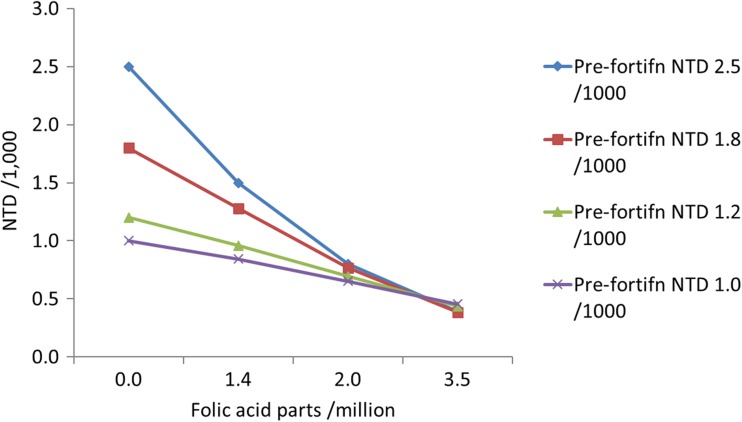
In the absence of intervention, early-onset congenital disorders lead to pregnancy loss, early death, or disability. Currently, lack of epidemiological data from many settings limits the understanding of the burden of these conditions, thus impeding health planning, policy-making, and commensurate resource allocation. The Modell Global Database of Congenital Disorders (MGDb) seeks to meet this need by combining general biological principles with observational and demographic data, to generate estimates of the burden of congenital disorders. A range of interventions along the life course can modify adverse outcomes associated with congenital disorders. Hence, access to and quality of services available for the prevention and care of congenital disorders affects both their birth prevalence and the outcomes for affected individuals. Information on this is therefore important to enable burden estimates for settings with limited observational data, but is lacking from many settings. This paper, the third in this special issue on methods used in the MGDb for estimating the global burden of congenital disorders, describes key interventions that impact on outcomes of congenital disorders and methods used to estimate their coverage where empirical data are not available.
Keywords: Access to care; Congenital malformations; Estimation; Interventions; Pregnancy outcomes.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Angastiniotis MA, Kyriakidou S, Hadjiminas M. How thalassaemia was controlled in Cyprus. World Health Forum. 1986;7:291–297.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
