

Microbiologic Diagnostic Workup of Acute Respiratory Failure with Pulmonary Infiltrates after Allogeneic Hematopoietic Stem Cell Transplantation: Findings in the Era of Molecular- and Biomarker-Based Assays
- PMID: 29550627
- PMCID: PMC7110883
- DOI: 10.1016/j.bbmt.2018.03.007
Microbiologic Diagnostic Workup of Acute Respiratory Failure with Pulmonary Infiltrates after Allogeneic Hematopoietic Stem Cell Transplantation: Findings in the Era of Molecular- and Biomarker-Based Assays
Abstract
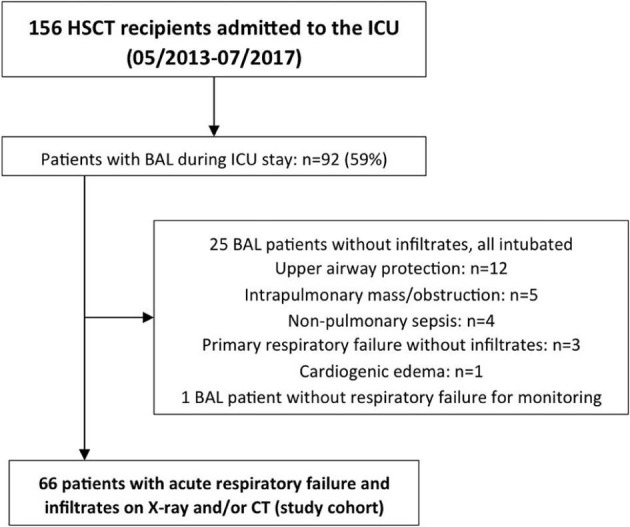
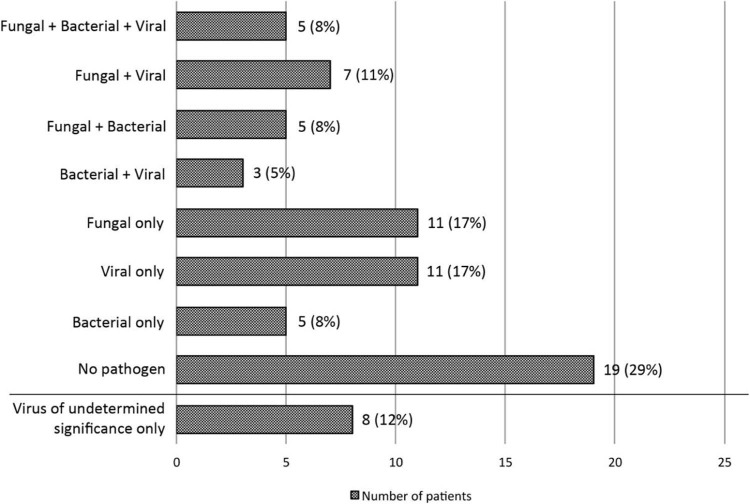
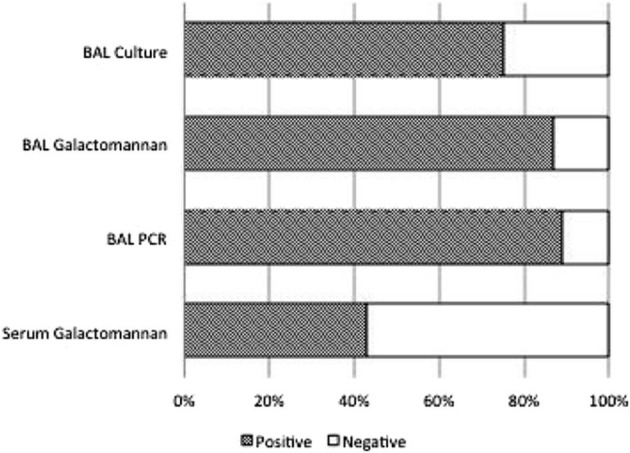
Allogeneic hematopoietic stem cell transplantation (HSCT) recipients frequently develop acute respiratory failure (ARF) with pulmonary infiltrates. Molecular- and biomarker-based assays enhance pathogen detection, but data on their yield in this population are scarce. This was a retrospective single-center study of 156 consecutive HSCT recipients admitted to the intensive care unit (ICU) between May 2013 and July 2017. Findings from a microbiologic diagnostic workup using currently available methods on bronchoalveolar lavage (BAL) and blood samples from 66 patients (age, 58 years [range, 45 to 64]; HSCT to ICU, 176 days [range, 85 to 407]) with ARF and pulmonary infiltrates were analyzed. In 47 patients (71%) a causative pathogen was identified (fungal, n = 28; viral, n = 26; bacterial, n = 18). Polymicrobial findings involving several pathogen groups occurred in 20 patients (30%). Culture (12/16, 75%), galactomannan (13/15, 87%), and Aspergillus-PCR (8/9, 89%) from BAL but not serum galactomannan (6/14, 43%) helped to diagnose invasive aspergillosis (n = 16, 24%). Aspergillus-PCR detected azole resistance in 2 cases. Mucorales was found in 7 patients (11%; BAL culture, n = 6; Mucorales-PCR, n = 1). Patients with identified pathogens had higher Simplified Acute Physiology Score II scores (P = .049) and inferior ICU survival (6% versus 37%, P < .01), which largely related to the presence of an invasive fungal infection. Eight patients (12%) had 1 or more viruses with uncertain lung pathogenicity as the sole microbiologic finding. A diagnostic microbiologic workup incorporating molecular- and biomarker-based assays identified pathogens in most HSCT recipients with ARF and pulmonary infiltrates admitted to the ICU. Implications of polymicrobial infection and pathogen patterns in these patients warrant further investigation.
Keywords: Acute respiratory failure; HSCT; Hematopoietic stem cell transplantation; ICU; Intensive care unit.
Copyright © 2018 The American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Lengline E., Chevret S., Moreau A.S. Changes in intensive care for allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transplant. 2015;50:840–845. - PubMed
-
- Azoulay E., Mokart D., Lambert J. Diagnostic strategy for hematology and oncology patients with acute respiratory failure: randomized controlled trial. Am J Respir Crit Care Med. 2010;182:1038–1046. - PubMed
-
- Schnell D., Mayaux J., Lambert J. Clinical assessment for identifying causes of acute respiratory failure in cancer patients. Eur Respir J. 2013;42:435–443. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
