

Secukinumab improves active psoriatic arthritis symptoms and inhibits radiographic progression: primary results from the randomised, double-blind, phase III FUTURE 5 study
- PMID: 29550766
- PMCID: PMC5965348
- DOI: 10.1136/annrheumdis-2017-212687
Secukinumab improves active psoriatic arthritis symptoms and inhibits radiographic progression: primary results from the randomised, double-blind, phase III FUTURE 5 study
Abstract
Objectives: To evaluate the effect of subcutaneous (s.c.) secukinumab, an interleukin-17A inhibitor, on clinical signs and symptoms and radiographic progression in patients with psoriatic arthritis (PsA).
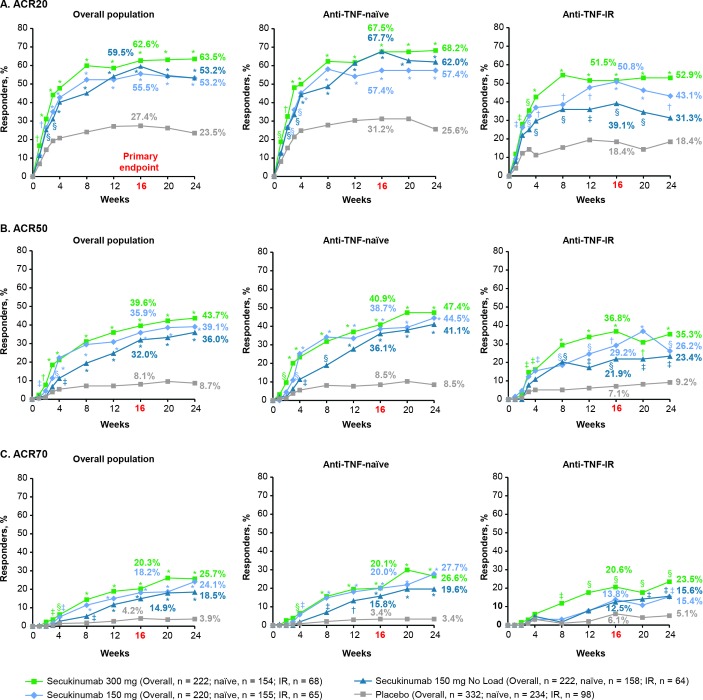
Methods: Adults (n=996) with active PsA were randomised 2:2:2:3 to s.c. secukinumab 300 mg or 150 mg with loading dose (LD), 150 mg without LD or placebo. All groups received secukinumab or placebo at baseline, weeks 1, 2 and 3 and then every 4 weeks from week 4. The primary endpoint was the proportion of patients achieving an American College of Rheumatology 20 (ACR20) response at week 16.
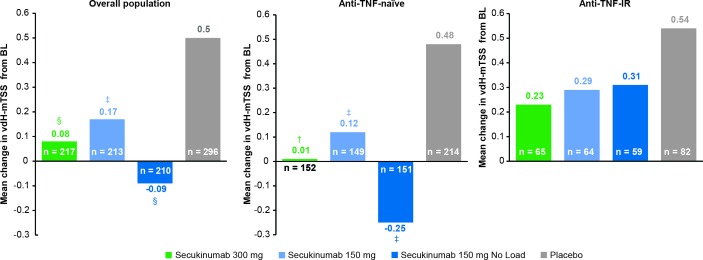
Results: Significantly more patients achieved an ACR20 response at week 16 with secukinumab 300 mg with LD (62.6%), 150 mg with LD (55.5%) or 150 mg without LD (59.5%) than placebo (27.4%) (p<0.0001 for all; non-responder imputation). Radiographic progression, as measured by van der Heijde-modified total Sharp score, was significantly inhibited at week 24 in all secukinumab arms versus placebo (p<0.01 for 300 mg with LD and 150 mg without LD and p<0.05 for 150 mg with LD; linear extrapolation). Adverse event rates at week 24 were similar across treatment arms: 63.1% (300 mg with LD), 62.7% (150 mg with LD), 61.1% (150 mg without LD) and 62.0% (placebo). No deaths or new safety signals were reported.
Conclusion: S.c. secukinumab 300 mg and 150 mg with and without LD significantly improved clinical signs and symptoms and inhibited radiographic structural progression versus placebo at week 24 in patients with PsA.
Trial registration number: NCT02404350; Results.
Keywords: cytokines; dmards (biologic); psoriatic arthritis; treatment.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: PM: Research grants from AbbVie, Amgen, BMS, Celgene, Janssen, Lilly, Novartis, Pfizer, SUN and UCB; consulting fees from AbbVie, Amgen, BMS, Celgene, Covagen, Crescendo, Janssen, LEO, Lilly, Merck, Novartis, Pfizer, SUN and UCB; speakers’ bureau for AbbVie, Amgen, BMS, Celgene, Genentech, Janssen, Lilly, Pfizer and UCB. DvdH: Consulting fees AbbVie, Amgen, Astellas, AstraZeneca, BMS, Boehringer Ingelheim, Celgene, Daiichi, Eli-Lilly, Galapagos, Gilead, Glaxo-Smith-Kline, Janssen, Merck, Novartis, Pfizer, Regeneron, Roche, Sanofi, Takeda, UCB. Director of Imaging Rheumatology. RL: Consultation or participation in advisory boards: Abbott/AbbVie, Ablynx, Amgen, Astra-Zeneca, Bristol-Myers Squibb, Centocor, GlaxoSmithKline, Novartis, Merck, Pfizer, Roche, Schering- Plough, UCB, Wyeth. Research grants: Abbott, Amgen, Centocor, Novartis, Pfizer, Roche, Schering-Plough, UCB, Wyeth. Speaker fees: Abbott, Amgen, Bristol-Myers Squibb, Centocor, Merck, Pfizer, Roche, Schering-Plough, UCB, Wyeth. RL: Director of Rheumatology Consultancy BV, which is a registered company under Dutch law. SM: Employee of Novartis, with Novartis stock. PR: Consulting fees for Abbott, AbbVie, Amgen, BMS, Celgene, Janssen, Novartis, Pfizer and Roche. Consultant to pharmaceutical companies dealing with biologic agents in rheumatology. HT: Consultation or participation in advisory boards: Abbvie, Novartis, Pfizer, UCB, Eli-Lilly, Janssen Education Grants: Novartis, Pfizer. AS: Research/Clinical trial grants from AbbVie, Gilead, Sanofi, Regeneron, Amgen, Roche, BMS, Janssen, Lilly, Novartis, Pfizer, UCB, Astra Zeneca, MedImmune, FujiFilm, Nichi-Iko, Mallinckrodt. Speakers’ bureau for AbbVie. EB: Consulting and speaking fees: Amgen, Roche, Eli Lilly, Pfizer, MSD, Novartis. SN: Consulting and speaker fees: Pfizer, Novartis, Astra-Zeneca, Janssen, Astellas, Roche. KM: Employee of Novartis, without Novartis stock. AR: Employee of Novartis, with Novartis stock. LP: Employee of Novartis, with Novartis stock. KA: Employee of Novartis, with Novartis stock.
Figures
Comment in
-
Are the loading dose treatment groups superior to the 150 mg without loading dose group in the secukinumab FUTURE 5 study?Ann Rheum Dis. 2019 Sep;78(9):e97. doi: 10.1136/annrheumdis-2018-213770. Epub 2018 May 31. Ann Rheum Dis. 2019. PMID: 29853450 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
