

Sirolimus in patients with clinically active systemic lupus erythematosus resistant to, or intolerant of, conventional medications: a single-arm, open-label, phase 1/2 trial
- PMID: 29551338
- PMCID: PMC5891154
- DOI: 10.1016/S0140-6736(18)30485-9
Sirolimus in patients with clinically active systemic lupus erythematosus resistant to, or intolerant of, conventional medications: a single-arm, open-label, phase 1/2 trial
Abstract
Background: Patients with systemic lupus erythematosus have T-cell dysfunction that has been attributed to the activation of the mammalian target of rapamycin (mTOR). Rapamycin inhibits antigen-induced T-cell proliferation and has been developed as a medication under the generic designation of sirolimus. We assessed safety, tolerance, and efficacy of sirolimus in a prospective, biomarker-driven, open-label clinical trial.
Methods: We did a single-arm, open-label, phase 1/2 trial of sirolimus in patients with active systemic lupus erythematosus disease unresponsive to, or intolerant of, conventional medications at the State University of New York Upstate Medical University (Syracuse, NY, USA). Eligible participants (aged ≥18 years) had active systemic lupus erythematosus fulfilling four or more of 11 diagnostic criteria defined by the American College of Rheumatology. We excluded patients with allergy or intolerance to sirolimus, patients with life-threatening manifestations of systemic lupus erythematosus, proteinuria, a urine protein to creatinine ratio higher than 0·5, anaemia, leucopenia, or thrombocytopenia. Patients received oral sirolimus at a starting dose of 2 mg per day, with dose adjusted according to tolerance and to maintain a therapeutic range of 6-15 ng/mL. Patients were treated with sirolimus for 12 months. Safety outcomes included tolerance as assessed by the occurrence of common side-effects. The primary efficacy endpoint was decrease in disease activity, assessed using the British Isles Lupus Assessment Group (BILAG) index and the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI). Blood samples of 56 matched healthy individuals were obtained as controls for immunobiological outcomes monitored at each visit. The primary efficacy endpoint was assessed in all patients who completed 12 months of treatment, and all patients who received at least one dose of treatment were included in the safety analyses. This trial is registered with ClinicalTrials.gov, number NCT00779194.
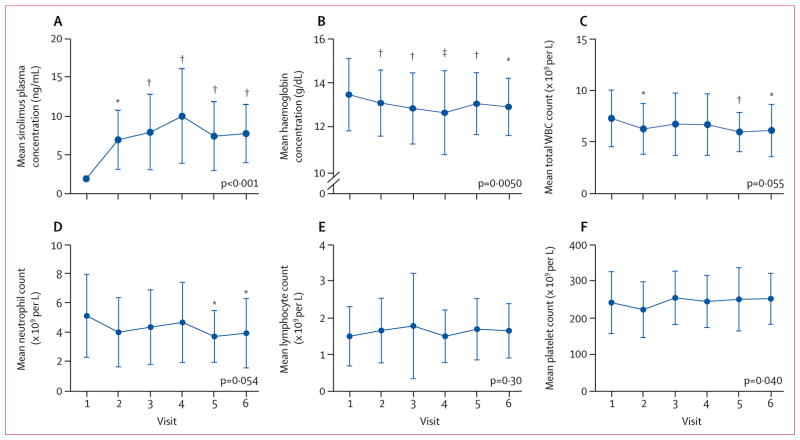
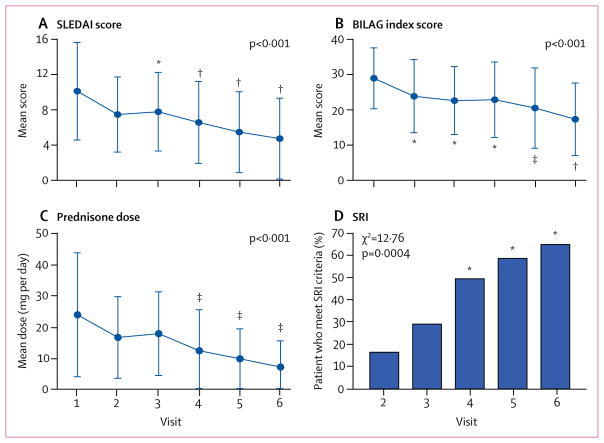
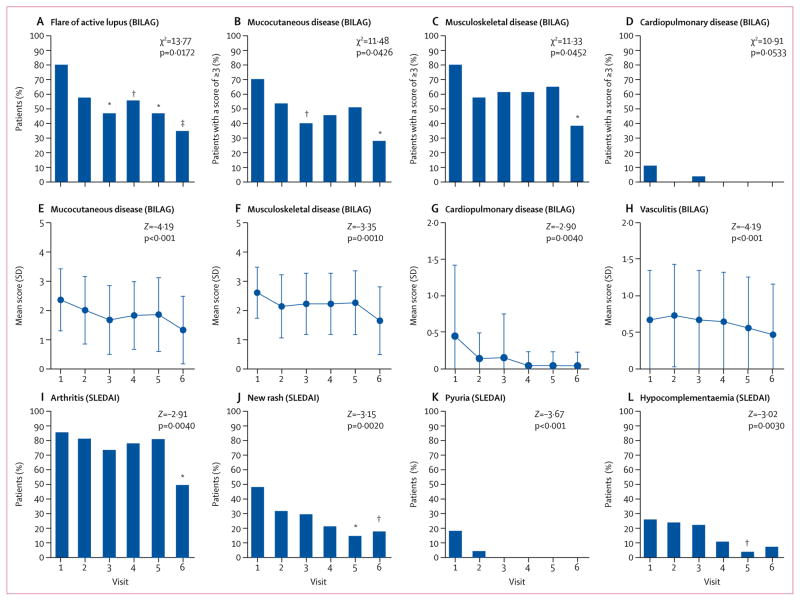
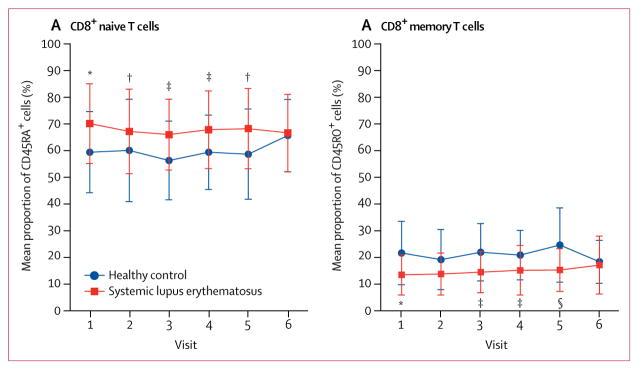
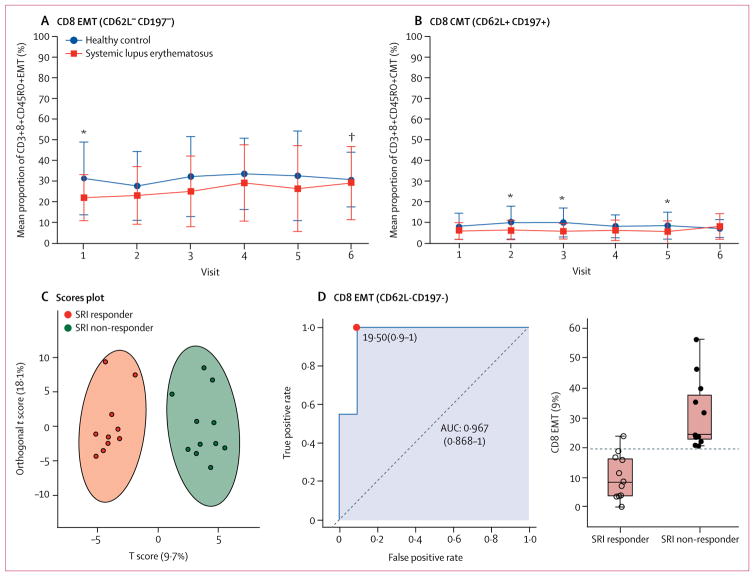
Findings: Between March 9, 2009, and Dec 8, 2014, 43 patients were enrolled, three of whom did not meet eligibility criteria. 11 of the 40 eligible patients discontinued study treatment because of intolerance (n=2) or non-compliance (n=9). SLEDAI and BILAG disease activity scores were reduced during 12 months of treatment in 16 (55%) of 29 patients who completed treatment. Mean SLEDAI score decreased from 10·2 (SD 5·6) at enrolment to 4·8 (4·5) after 12 months of treatment (p<0·001) and the mean total BILAG index score decreased from 28·4 (12·4) at enrolment to 17·4 (10·7) after 12 months of treatment (p<0·001). The mean daily dose of prednisone required to control disease activity decreased from 23·7 mg (SD 9·6) to 7·2 mg (2·3; p<0·001) after 12 months of treatment. Sirolimus expanded CD4+CD25+FoxP3+ regulatory T cells and CD8+ memory T-cell populations and inhibited interleukin-4 and interleukin-17 production by CD4+ and CD4-CD8- double-negative T cells after 12 months. CD8+ memory T cells were selectively expanded in SRI-responders. Patient liver function and lymphocyte counts were unchanged. Although HDL-cholesterol (Z=-2·50, p=0·012), neutrophil counts (Z=-1·92, p=0·054), and haemoglobin (Z=-2·83, p=0·005) were moderately reduced during treatment, all changes occurred within a range that was considered safe. Platelet counts were slightly elevated during treatment (Z=2·06, p=0·0400).
Interpretation: These data show that a progressive improvement in disease activity is associated with correction of pro-inflammatory T-cell lineage specification in patients with active systemic lupus erythematosus during 12 months of sirolimus treatment. Follow-up placebo-controlled clinical trials in diverse patient populations are warranted to further define the role of mTOR blockade in treatment of systemic lupus erythematosus.
Funding: Pfizer, the National Institutes of Health, and the Central New York Community Foundation.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We declare no competing interests.
Figures
Comment in
-
CD8 T cells and mTOR: new concepts and targets for systemic lupus erythematosus.Lancet. 2018 Mar 24;391(10126):1126-1127. doi: 10.1016/S0140-6736(18)30544-0. Epub 2018 Mar 15. Lancet. 2018. PMID: 29551336 No abstract available.
-
Sirolimus for systemic lupus erythematosus.Lancet. 2018 Sep 1;392(10149):733-734. doi: 10.1016/S0140-6736(18)31792-6. Lancet. 2018. PMID: 30191825 No abstract available.
-
Sirolimus for systemic lupus erythematosus - Authors' reply.Lancet. 2018 Sep 1;392(10149):734. doi: 10.1016/S0140-6736(18)31794-X. Lancet. 2018. PMID: 30191826 No abstract available.
-
Is sirolimus a treatment option for patients with systemic lupus erythematosus?Clin Exp Rheumatol. 2019 Nov-Dec;37 Suppl 122(6):13. Epub 2019 Jul 12. Clin Exp Rheumatol. 2019. PMID: 31376256 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
