

Autoantibodies May Predict Immune-Related Toxicity: Results from a Phase I Study of Intralesional Bacillus Calmette-Guérin followed by Ipilimumab in Patients with Advanced Metastatic Melanoma
- PMID: 29552014
- PMCID: PMC5840202
- DOI: 10.3389/fimmu.2018.00411
Autoantibodies May Predict Immune-Related Toxicity: Results from a Phase I Study of Intralesional Bacillus Calmette-Guérin followed by Ipilimumab in Patients with Advanced Metastatic Melanoma
Abstract
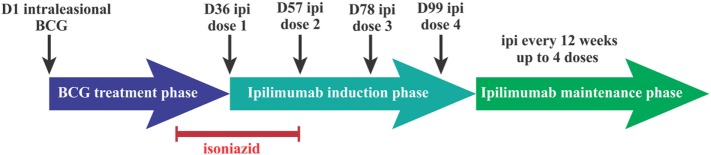
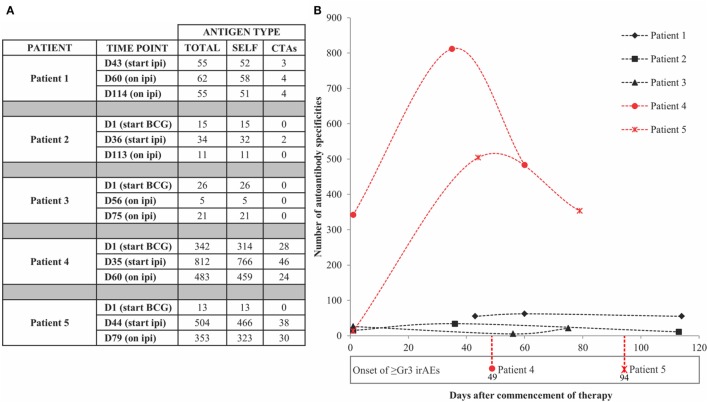
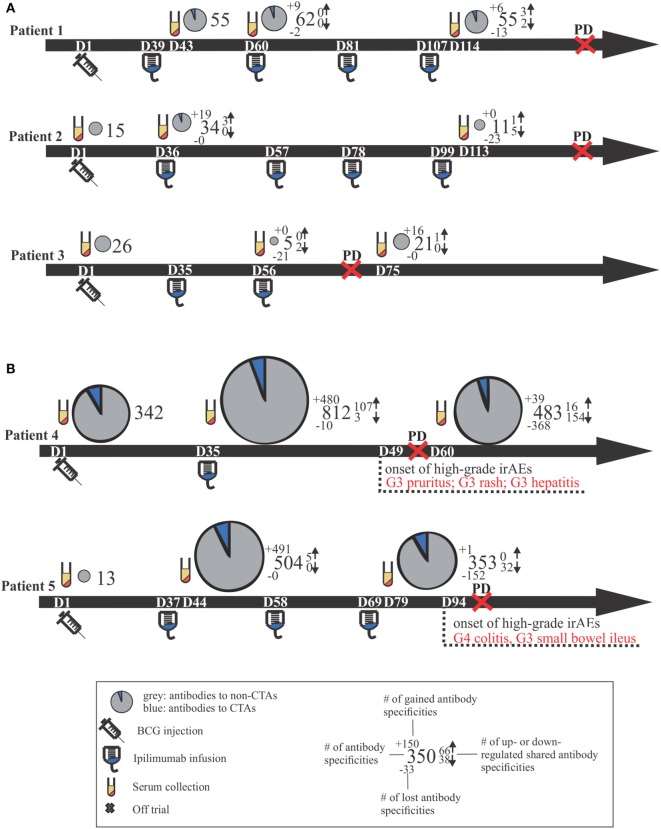
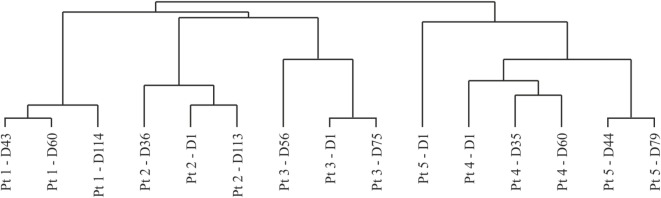
Immune checkpoint inhibitors (ICIs) have revolutionized the treatment of advanced melanoma. The first ICI to demonstrate clinical benefit, ipilimumab, targets cytotoxic T-lymphocyte-associated antigen-4 (CTLA-4); however, the long-term overall survival is just 22%. More than 40 years ago intralesional (IL) bacillus Calmette-Guérin (BCG), a living attenuated strain of Mycobacterium bovis, was found to induce tumor regression by stimulating cell-mediated immunity following a localized and self-limiting infection. We evaluated these two immune stimulants in combination with melanoma with the aim of developing a more effective immunotherapy and to assess toxicity. In this phase I study, patients with histologically confirmed stage III/IV metastatic melanoma received IL BCG injection followed by up to four cycles of intravenous ipilimumab (anti-CTLA-4) (ClinicalTrials.gov number NCT01838200). The trial was discontinued following treatment of the first five patients as the two patients receiving the escalation dose of BCG developed high-grade immune-related adverse events (irAEs) typical of ipilimumab monotherapy. These irAEs were characterized in both patients by profound increases in the repertoire of autoantibodies directed against both self- and cancer antigens. Interestingly, the induced autoantibodies were detected at time points that preceded the development of symptomatic toxicity. There was no overlap in the antigen specificity between patients and no evidence of clinical responses. Efforts to increase response rates through the use of novel immunotherapeutic combinations may be associated with higher rates of irAEs, thus the imperative to identify biomarkers of toxicity remains strong. While the small patient numbers in this trial do not allow for any conclusive evidence of predictive biomarkers, the observed changes warrant further examination of autoantibody repertoires in larger patient cohorts at risk of developing irAEs during their course of treatment. In summary, dose escalation of IL BCG followed by ipilimumab therapy was not well tolerated in advanced melanoma patients and showed no evidence of clinical benefit. Measuring autoantibody responses may provide early means for identifying patients at risk from developing severe irAEs during cancer immunotherapy.
Keywords: bacillus Calmette–Guerin; immune-related adverse events; ipilimumab; melanoma; protein microarrays.
Figures
Similar articles
-
Ipilimumab targeting CD28-CTLA-4 axis: new hope in the treatment of melanoma.Curr Top Med Chem. 2012;12(1):61-6. doi: 10.2174/156802612798919231. Curr Top Med Chem. 2012. PMID: 22196270 Review.
-
Autoantibody Development under Treatment with Immune-Checkpoint Inhibitors.Cancer Immunol Res. 2019 Jan;7(1):6-11. doi: 10.1158/2326-6066.CIR-18-0245. Epub 2018 Nov 13. Cancer Immunol Res. 2019. PMID: 30425107
-
Clinical and molecular insights into BCG immunotherapy for melanoma.J Intern Med. 2020 Dec;288(6):625-640. doi: 10.1111/joim.13037. Epub 2020 Mar 4. J Intern Med. 2020. PMID: 32128919 Review.
-
Combining a Universal Telomerase Based Cancer Vaccine With Ipilimumab in Patients With Metastatic Melanoma - Five-Year Follow Up of a Phase I/IIa Trial.Front Immunol. 2021 May 11;12:663865. doi: 10.3389/fimmu.2021.663865. eCollection 2021. Front Immunol. 2021. PMID: 34046035 Free PMC article. Clinical Trial.
-
Development of Bell's Palsy After Treatment With Ipilimumab and Nivolumab for Metastatic Melanoma: A Case Report.J Immunother. 2018 Jan;41(1):39-41. doi: 10.1097/CJI.0000000000000184. J Immunother. 2018. PMID: 28926356
Cited by
-
Insights into the Molecular Mechanisms Behind Intralesional Immunotherapies for Advanced Melanoma.Cancers (Basel). 2020 May 22;12(5):1321. doi: 10.3390/cancers12051321. Cancers (Basel). 2020. PMID: 32455916 Free PMC article. Review.
-
Association between Changes in the Patterns of Antinuclear Autoantibodies during Immune Checkpoint Inhibition Therapy and the Development of Severe Immune Related Adverse Events.Int J Mol Sci. 2022 Oct 20;23(20):12641. doi: 10.3390/ijms232012641. Int J Mol Sci. 2022. PMID: 36293498 Free PMC article.
-
Perspective: cancer vaccines in the era of immune checkpoint blockade.Mamm Genome. 2018 Dec;29(11-12):703-713. doi: 10.1007/s00335-018-9786-z. Epub 2018 Nov 16. Mamm Genome. 2018. PMID: 30446791 Free PMC article. Review.
-
Cytokines, Chemokines, and Other Biomarkers of Response for Checkpoint Inhibitor Therapy in Skin Cancer.Front Med (Lausanne). 2018 Dec 12;5:351. doi: 10.3389/fmed.2018.00351. eCollection 2018. Front Med (Lausanne). 2018. PMID: 30631766 Free PMC article. Review.
-
A proteome-wide immuno-mass spectrometric identification of serum autoantibodies.Clin Proteomics. 2019 Jun 20;16:25. doi: 10.1186/s12014-019-9246-0. eCollection 2019. Clin Proteomics. 2019. PMID: 31249498 Free PMC article.
References
-
- Sanderson K, Scotland R, Lee P, Liu D, Groshen S, Snively J, et al. Autoimmunity in a phase I trial of a fully human anti-cytotoxic T-lymphocyte antigen-4 monoclonal antibody with multiple melanoma peptides and montanide ISA 51 for patients with resected stages III and IV melanoma. J Clin Oncol (2005) 23(4):741–50.10.1200/JCO.2005.01.128 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical