

Who will benefit more from maintenance therapy of metastatic colorectal cancer?
- PMID: 29552327
- PMCID: PMC5844763
- DOI: 10.18632/oncotarget.23549
Who will benefit more from maintenance therapy of metastatic colorectal cancer?
Abstract
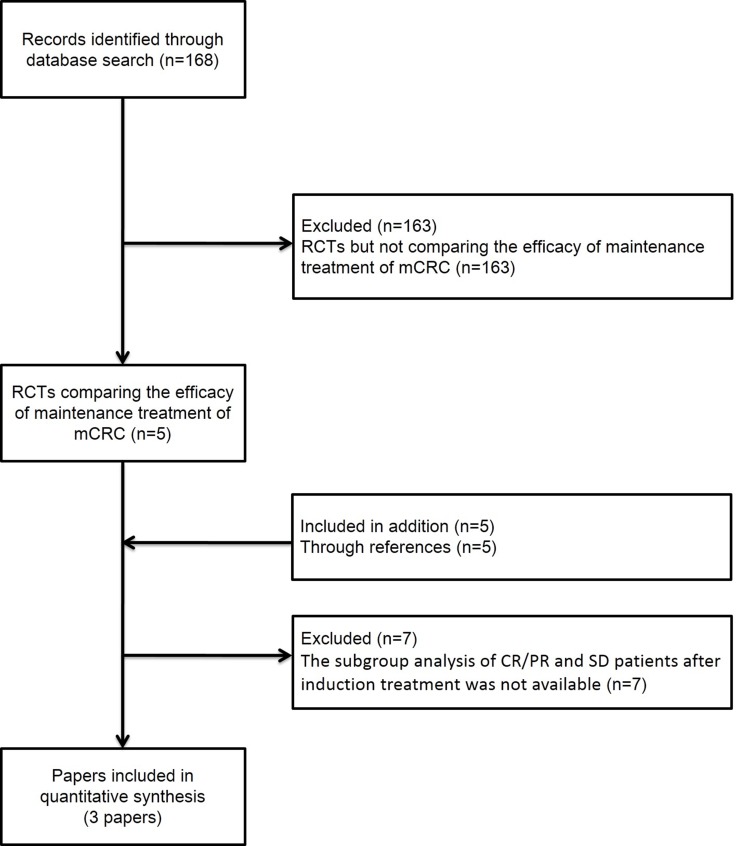
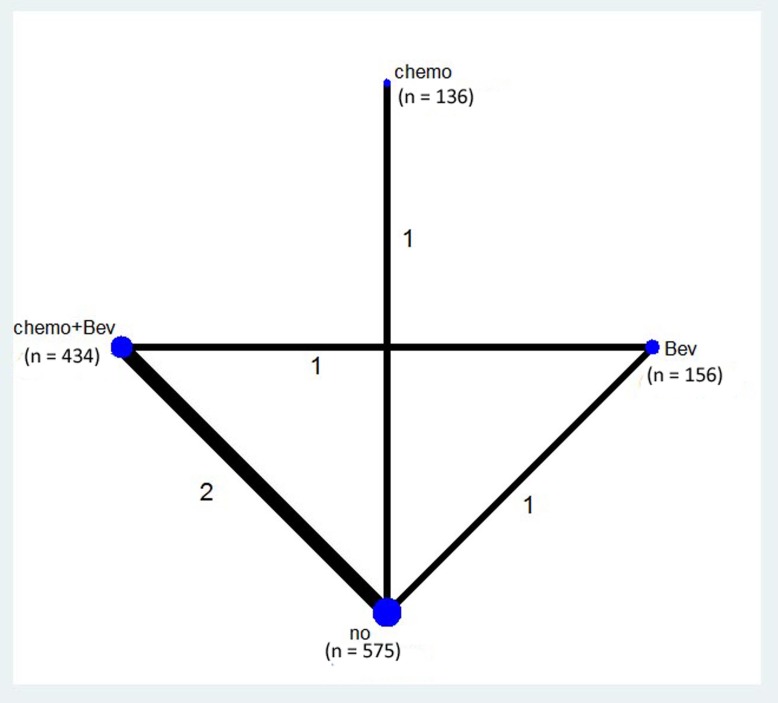
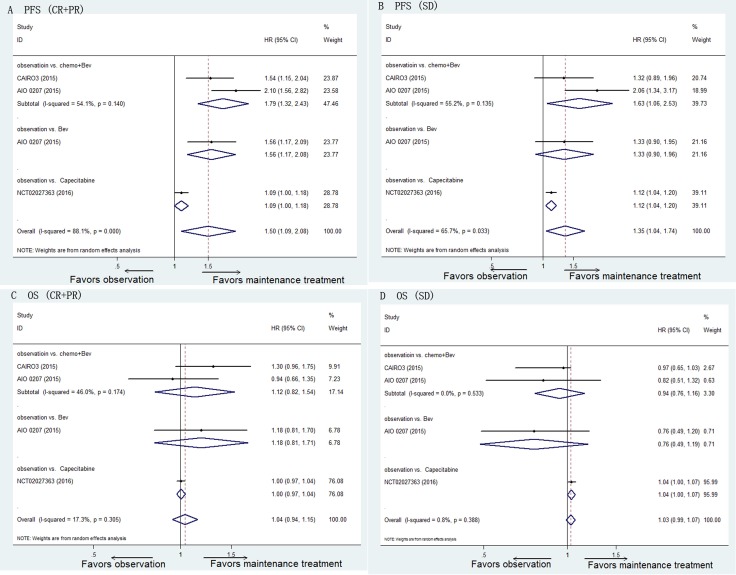
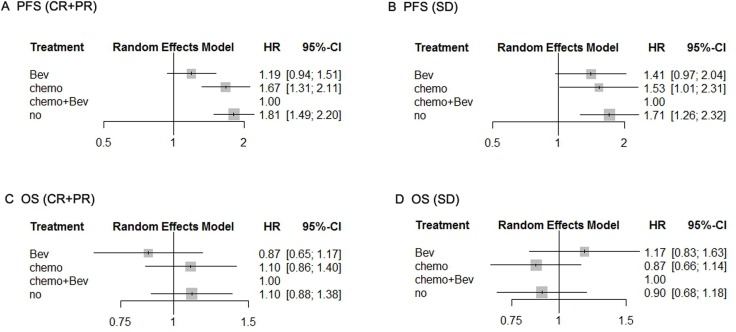
Whether there is a difference in the efficacy of maintenance treatment for metastatic colorectal cancer (mCRC) between patients who achieve complete response (CR)/partial response (PR) and those with stable disease (SD) after induction treatment is controversial. PubMed, Cochrane Systematic Reviews, the Cochrane Collaboration Central Register of Controlled Clinical Trials, ClinicalTrials.gov, and databases of conferences were queried to identify randomized controlled trials evaluating the efficacy of maintenance treatment for mCRC patients. The search included articles dated from the inception of these resources until June 20, 2017. We estimated hazard ratios (HRs) for progression-free survival (PFS) and overall survival (OS). Network meta-analysis was performed to compare the efficacy of four regimens as maintenance treatment. Three randomized controlled trials comprising 1,301 patients were included in this network meta-analysis. Patients who achieved CR/PR after induction therapy benefited more from maintenance treatment than patients who achieved SD (PFS: HR [CR/PR] 1.50, 95% CI 1.09-2.08, vs. HR [SD] 1.35, 95% CI 1.04-1.74; OS: HR [CR/PR] 1.04, 95% CI 0.94-1.15, vs. HR [SD] 1.03, 95% CI 0.99-1.07). The results of network meta-analysis suggested that chemotherapy alone and observation were inferior to chemotherapy plus bevacizumab as maintenance treatment. Patients with mCRC who achieve CR/PR after induction therapy might benefit more from maintenance treatment than those with SD. Chemotherapy plus bevacizumab was the most appropriate regimen for maintenance treatment.
Keywords: complete or partial response; maintenance treatment; metastatic colorectal cancer; network meta-analysis; stable disease.
Conflict of interest statement
CONFLICTS OF INTEREST There is no conflicts of interest.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin. 2017;67:7–30. https://doi.org/10.3322/caac.21387. - DOI - PubMed
-
- Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–32. https://doi.org/10.3322/caac.21338. - DOI - PubMed
-
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1) Eur J Cancer. 2009;45:228–47. https://doi.org/10.1016/j.ejca.2008.10.026S0959-8049(08)00873-3. - DOI - PubMed
-
- Simkens LH, van Tinteren H, May A, ten Tije AJ, Creemers GJ, Loosveld OJ, de Jongh FE, Erdkamp FL, Erjavec Z, van der Torren AM, Tol J, Braun HJ, Nieboer P, et al. Maintenance treatment with capecitabine and bevacizumab in metastatic colorectal cancer (CAIRO3): a phase 3 randomised controlled trial of the Dutch Colorectal Cancer Group. Lancet. 2015;385:1843–52. https://doi.org/10.1016/S0140-6736(14)62004-3S0140-6736(14)62004-3. - DOI - PubMed
-
- Hegewisch-Becker S, Graeven U, Lerchenmuller CA, Killing B, Depenbusch R, Steffens CC, Al-Batran SE, Lange T, Dietrich G, Stoehlmacher J, Tannapfel A, Reinacher-Schick A, Quidde J, et al. Maintenance strategies after first-line oxaliplatin plus fluoropyrimidine plus bevacizumab for patients with metastatic colorectal cancer (AIO 0207): a randomised, non-inferiority, open-label, phase 3 trial. Lancet Oncol. 2015;16:1355–69. https://doi.org/10.1016/S1470-2045(15)00042-XS1470-2045(15)00042-X. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
