

Surgical Management of the Multiple-Ligament Knee Injury
- PMID: 29552481
- PMCID: PMC5851650
- DOI: 10.1016/j.eats.2017.08.079
Surgical Management of the Multiple-Ligament Knee Injury
Abstract
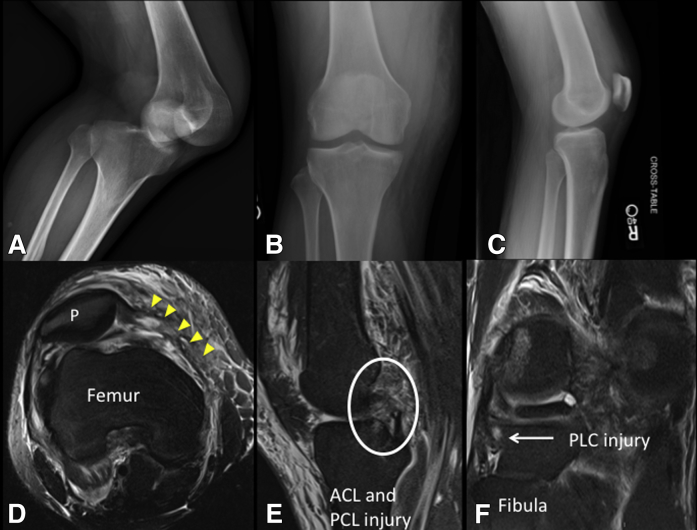
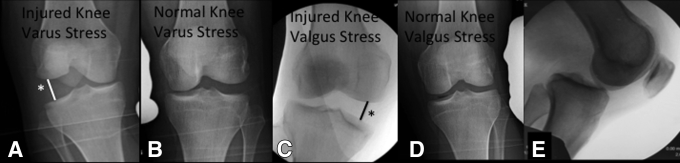
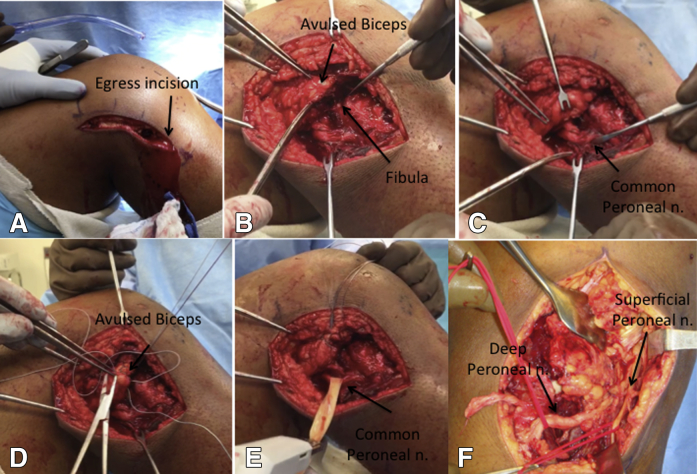
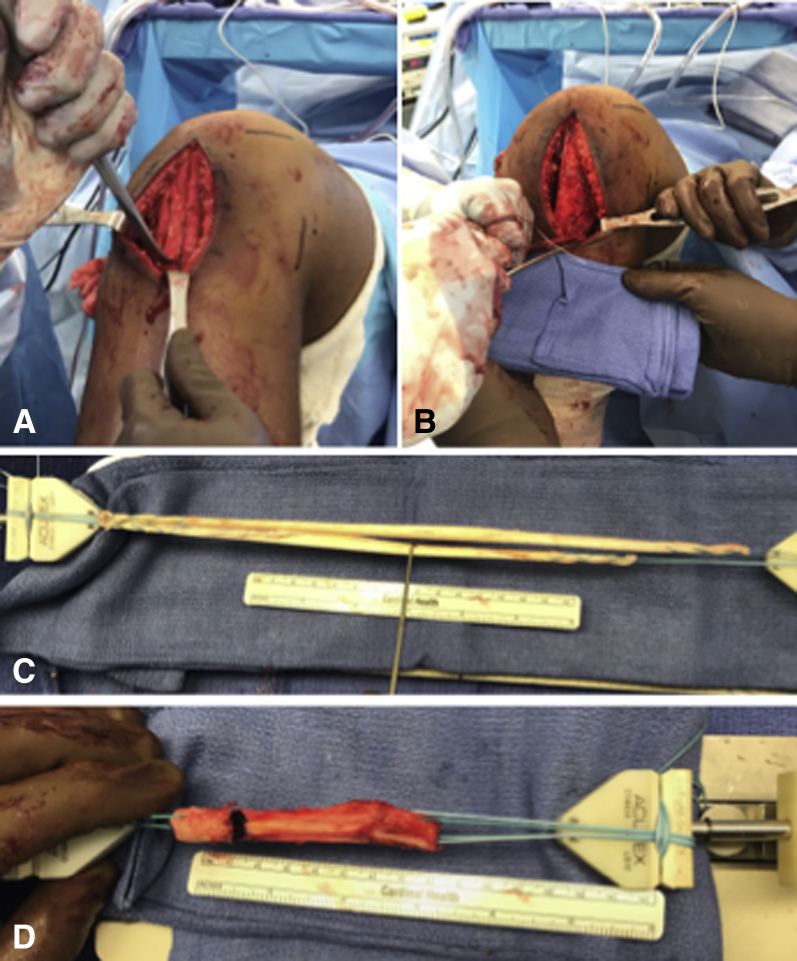
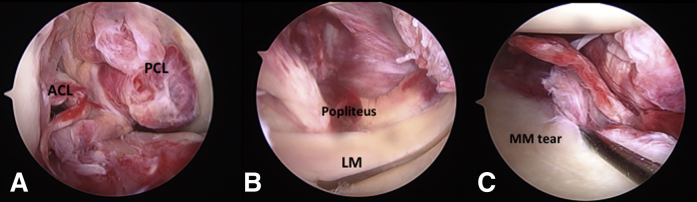
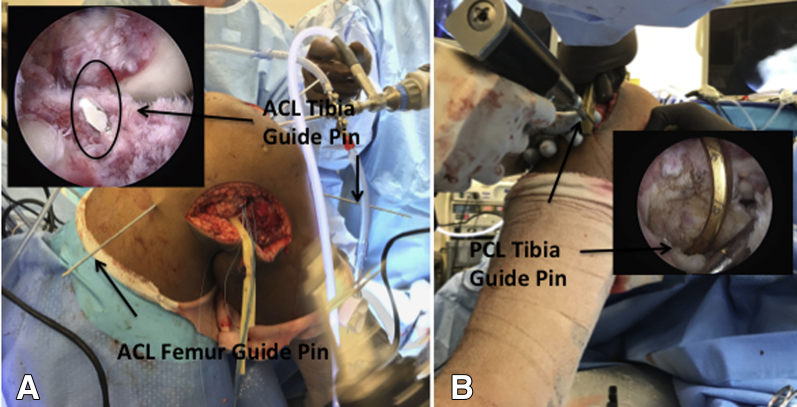
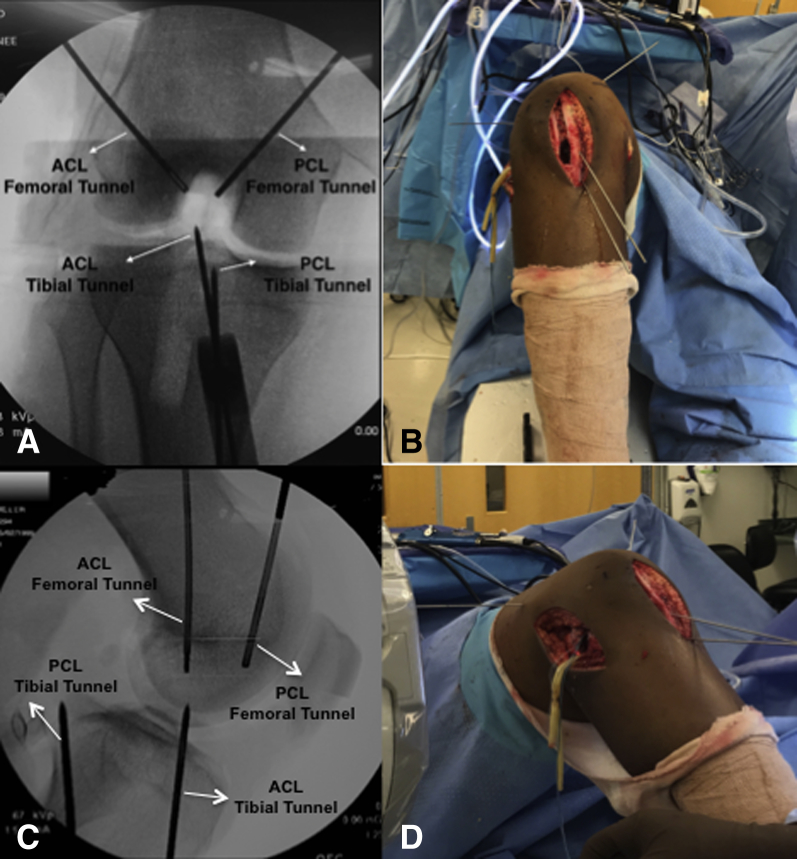
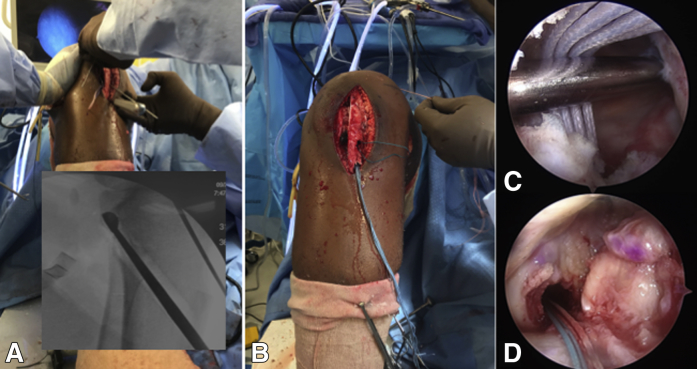
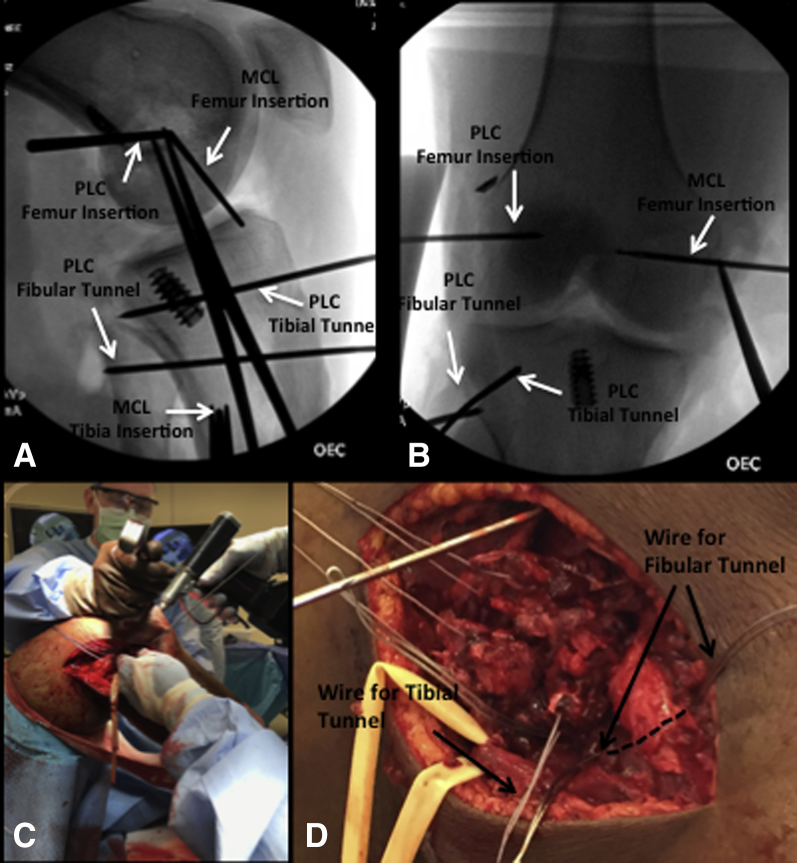
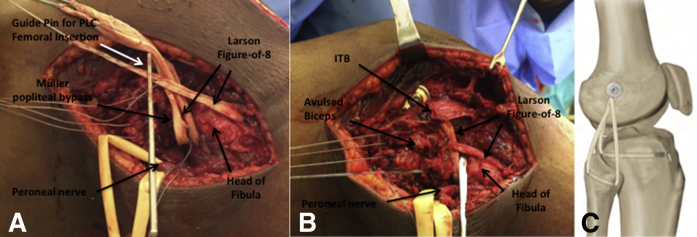
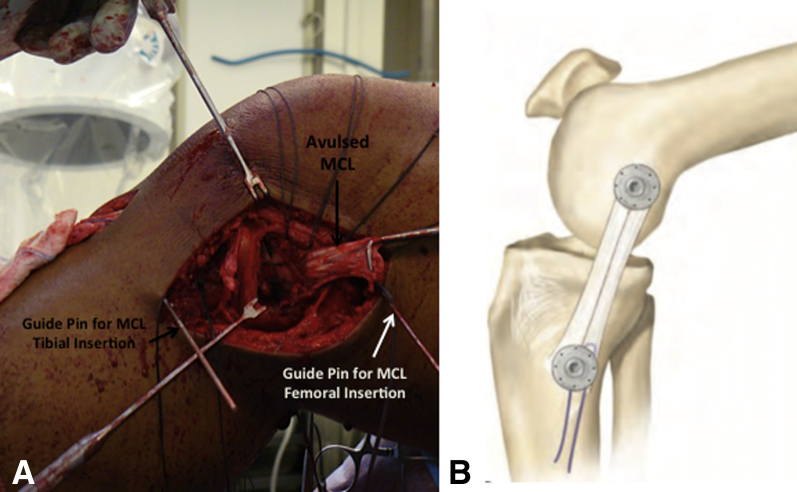
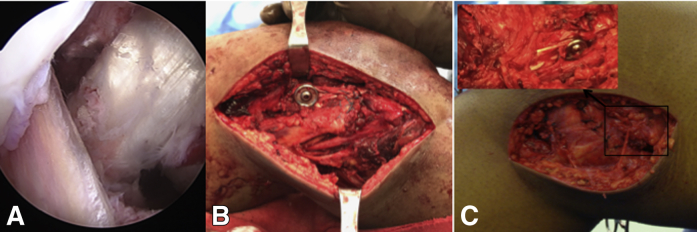
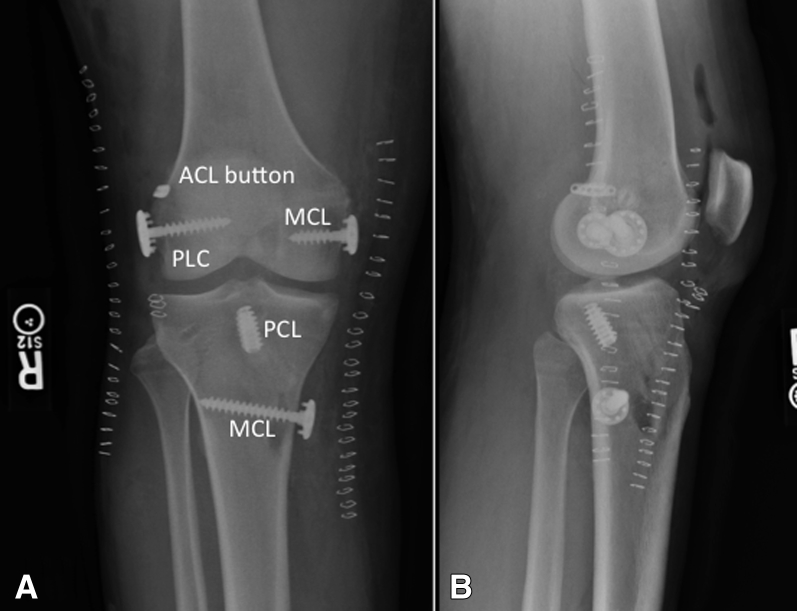
The management of multiligament knee injury is a complex process starting with the adequate identification of the injury. A detailed physical and radiographic examination with a thorough understanding of knee anatomy is crucial to assess all damaged structures: anterior cruciate ligament, posterior cruciate ligament, posteromedial corner including the medial collateral ligament, and posterolateral corner including the lateral collateral ligament. Several surgical techniques have been developed throughout the years to adequately address these ligament insufficiencies. In this surgical technique description, we describe a reproducible method for the assessment and surgical management of a knee dislocation (KDIV) injury. Our approach includes using anatomic single-bundle cruciate ligament reconstructions with modified Bosworth technique for medial-side injuries and a combination of Müller popliteal bypass and Larson figure-of-8 techniques for posterolateral corner injuries. The orders of surgical steps is described concisely, and technical controversies such as graft choice, tunnel positioning, and sequence of graft fixation are discussed in detail.
Figures
Similar articles
-
Multiligament Reconstruction of the Knee in the Setting of Knee Dislocation With a Medial-Sided Injury.Arthrosc Tech. 2017 Mar 20;6(2):e341-e350. doi: 10.1016/j.eats.2016.10.003. eCollection 2017 Apr. Arthrosc Tech. 2017. PMID: 28580251 Free PMC article.
-
The Posteromedial Corner of the Knee: Anatomy, Pathology, and Management Strategies.J Am Acad Orthop Surg. 2017 Nov;25(11):752-761. doi: 10.5435/JAAOS-D-16-00020. J Am Acad Orthop Surg. 2017. PMID: 29059112 Review.
-
Reconstruction of the Posterolateral Corner After Sequential Sectioning Restores Knee Kinematics.Orthop J Sports Med. 2015 Feb 12;3(2):2325967115570560. doi: 10.1177/2325967115570560. eCollection 2015 Feb. Orthop J Sports Med. 2015. PMID: 26535381 Free PMC article.
-
Multiple Ligament Reconstructions of the Knee and Posterolateral Corner.Arthrosc Tech. 2021 Apr 12;10(5):e1269-e1280. doi: 10.1016/j.eats.2021.01.024. eCollection 2021 May. Arthrosc Tech. 2021. PMID: 34141542 Free PMC article.
-
Physical examination and imaging of the medial collateral ligament and posteromedial corner of the knee.Sports Med Arthrosc Rev. 2006 Jun;14(2):67-73. doi: 10.1097/01.jsa.0000212303.57625.47. Sports Med Arthrosc Rev. 2006. PMID: 17135949 Review.
Cited by
-
Modern Treatment Principles for Multiligament Knee Injuries.Arch Bone Jt Surg. 2022 Nov;10(11):937-950. doi: 10.22038/ABJS.2021.60188.2971. Arch Bone Jt Surg. 2022. PMID: 36561221 Free PMC article. Review.
-
Strategies for Preventing Tunnel Convergence in Multiligament Knee Injury Reconstructions.Indian J Orthop. 2024 Oct 14;58(11):1528-1536. doi: 10.1007/s43465-024-01267-4. eCollection 2024 Nov. Indian J Orthop. 2024. PMID: 39539327 Review.
-
Single-stage versus two-stage reconstruction in chronic multi ligament knee injury.Int J Burns Trauma. 2022 Apr 15;12(2):35-44. eCollection 2022. Int J Burns Trauma. 2022. PMID: 35620740 Free PMC article.
-
Clinical Effectiveness of Arthroscopy-Assisted Fixation in the Treatment of Avulsed Posterior Cruciate Ligament Injuries.Cureus. 2023 Dec 8;15(12):e50152. doi: 10.7759/cureus.50152. eCollection 2023 Dec. Cureus. 2023. PMID: 38186527 Free PMC article. Review.
-
Complications of surgical reconstruction of multiligament injuries of the knee joint: diagnosis, prevention and treatment.EFORT Open Rev. 2021 Oct 19;6(10):973-981. doi: 10.1302/2058-5241.6.210057. eCollection 2021 Oct. EFORT Open Rev. 2021. PMID: 34760296 Free PMC article. Review.
References
-
- Levy B.A., Dajani K.A., Whelan D.B. Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthroscopy. 2009;25:430–438. - PubMed
-
- Fanelli G.C. Surgical treatment of lateral posterolateral instability of the knee using biceps tendon procedures. Sports Med Arthrosc. 2006;14:37–43. - PubMed
-
- Stannard J.P., Brown S.L., Farris R.C., McGwin G., Jr., Volgas D.A. The posterolateral corner of the knee: repair versus reconstruction. Am J Sports Med. 2005;33:881–888. - PubMed
-
- LaPrade R.F., Johansen S., Wentorf F.A., Engebretsen L., Esterberg J.L., Tso A. An analysis of an anatomical posterolateral knee reconstruction: an in vitro biomechanical study and development of a surgical technique. Am J Sports Med. 2004;32:1405–1414. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
