

Septic Arthritis After Anterior Cruciate Ligament Reconstruction: Clinical and Functional Outcomes Based on Graft Retention or Removal
- PMID: 29552571
- PMCID: PMC5846937
- DOI: 10.1177/2325967118758626
Septic Arthritis After Anterior Cruciate Ligament Reconstruction: Clinical and Functional Outcomes Based on Graft Retention or Removal
Abstract
Background: There remains a debate over whether to retain the index anterior cruciate ligament (ACL) graft in the setting of septic arthritis.
Purpose: To evaluate and compare clinical outcomes for the treatment of septic arthritis after ACL reconstruction (ACLR) in those with and without early graft retention.
Study design: Case series; Level of evidence, 4.
Methods: The Military Health System was queried for all ACLR procedures performed between 2007 and 2013. Inclusion criteria required active military status, primary ACLR with secondary septic arthritis, and minimum 24-month surveillance. Demographic, clinical, and surgical variables were evaluated using descriptive statistics and regression analysis for factors influencing selected outcomes.
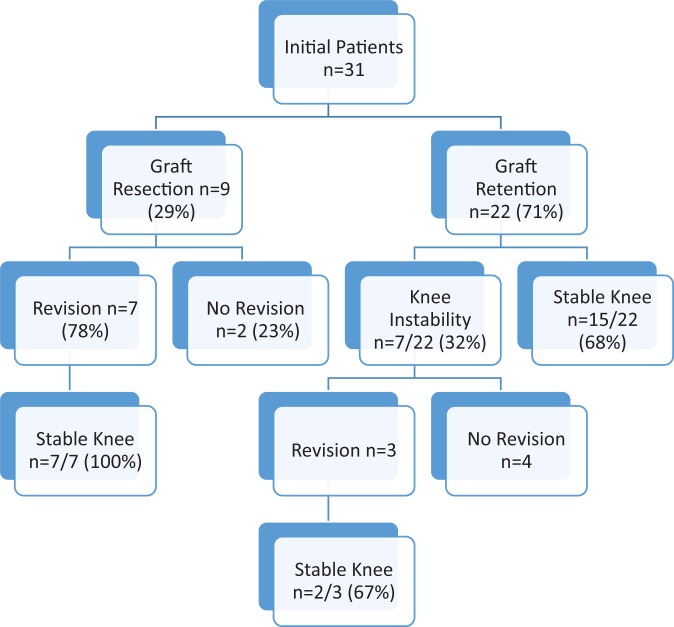
Results: Of 9511 ACLR procedures, 31 (0.32%) were identified as having secondary septic arthritis requiring urgent arthroscopic irrigation and debridement and intravenous antibiotics (mean, 6.3 weeks). The majority (62%) were treated in the subacute (2 weeks to 2 months) setting. Index ACLR was performed with a hamstring autograft (n = 17, 55%), soft tissue allograft (n = 11, 35%), and patellar tendon autograft (n = 3, 10%). The graft was retained in 71% (n = 22) of patients, while 29% (n = 9) underwent early graft debridement. At a mean 26.9-month follow-up, 48% of patients (n = 15) had returned to the military. Graft removal was not predictive of return to active duty (P = .29). The presence of postoperative complications, including symptomatic postinfection arthritis (22.6%) and arthrofibrosis (9.7%), was the only variable predictive of inability to return to duty (odds ratio, 27.5 [95% CI, 3.24-233.47]; P = .002). Seven of 9 patients who underwent graft debridement underwent revision ACLR, and all 7 had stable knees at final follow-up compared with 68% (15/22) in the graft retention group.
Conclusion: Arthroscopic debridement with early graft removal and staged revision ACLR remains a viable option for restoring knee stability (100%), although the rate of return to active duty was low in the graft resection group (33%). The risk of knee laxity did not differ based on early graft retention. Time to presentation with graft retention was not associated with a decreased rate of graft laxity.
Keywords: anterior cruciate ligament; anterior cruciate ligament reconstruction; laxity; septic arthritis.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: B.R.W. receives publishing royalties from Elsevier and is a paid consultant for Genzyme. B.D.O. is a paid consultant for Conmed Linvatec, Mitek, and the Musculoskeletal Research Foundation; receives research support from Histogenics; and receives publishing royalties from Saunders/Mosby-Elsevier and Springer.
Figures
References
-
- Benner RW, Shelbourne KD, Freeman H. Infections and patellar tendon ruptures after anterior cruciate ligament reconstruction: a comparison of ipsilateral and contralateral patellar tendon autografts. Am J Sports Med. 2011;39(3):519–525. - PubMed
-
- Bostrom Windhamre H, Mikkelsen C, Forssblad M, Willberg L. Postoperative septic arthritis after anterior cruciate ligament reconstruction: does it affect the outcome? A retrospective controlled study. Arthroscopy. 2014;30(9):1100–1109. - PubMed
-
- Burks RT, Friederichs MG, Fink B, Luker MG, West HS, Greis PE. Treatment of postoperative anterior cruciate ligament infections with graft removal and early reimplantation. Am J Sports Med. 2003;31(3):414–418. - PubMed
-
- Cadet ER, Makhni EC, Mehran N, Schulz BM. Management of septic arthritis following anterior cruciate ligament reconstruction: a review of current practices and recommendations. J Am Acad Orthop Surg. 2013;21(11):647–656. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
