

Porphyria: What Is It and Who Should Be Evaluated?
- PMID: 29553924
- PMCID: PMC5916231
- DOI: 10.5041/RMMJ.10333
Porphyria: What Is It and Who Should Be Evaluated?
Abstract
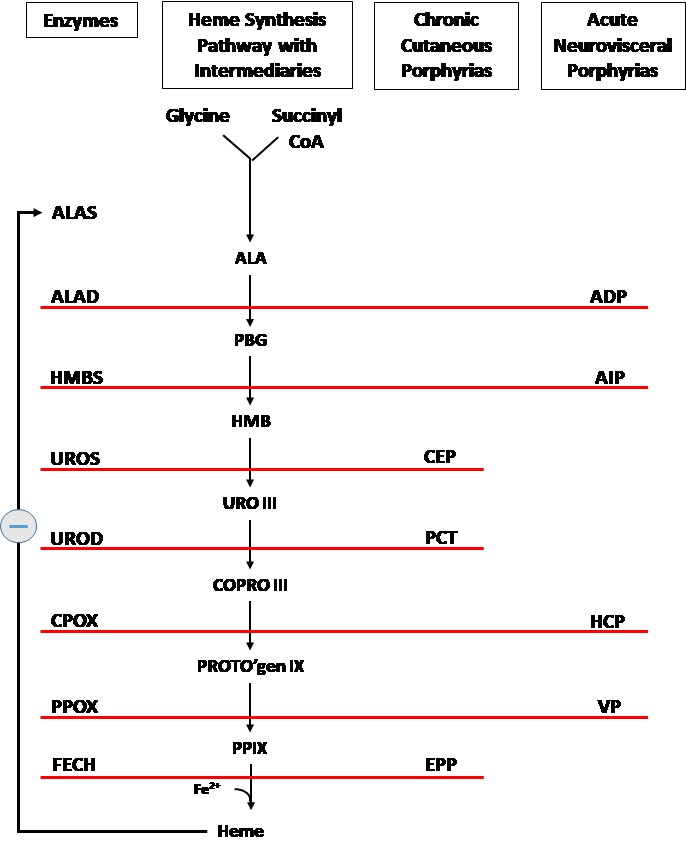
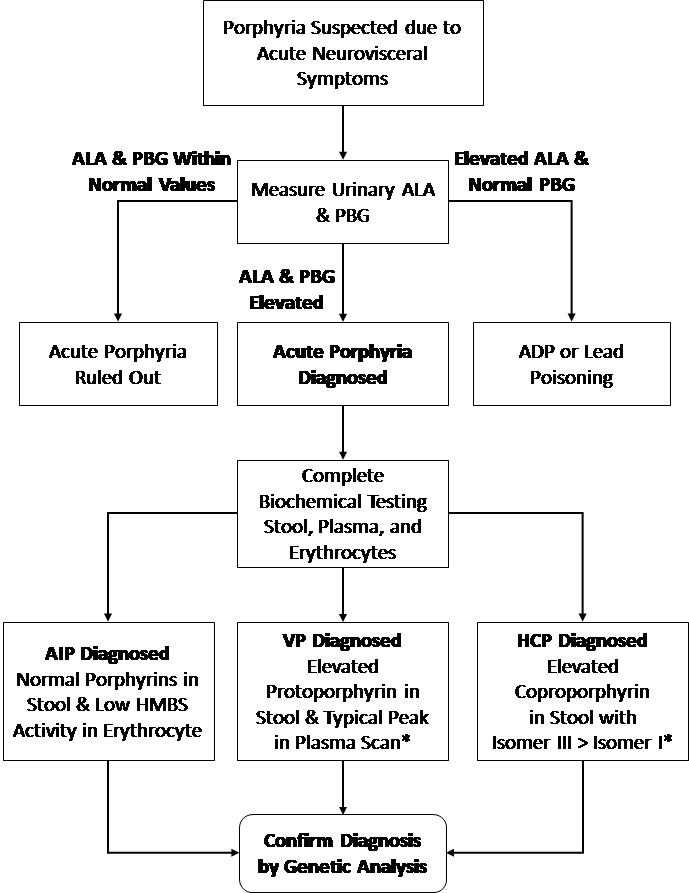
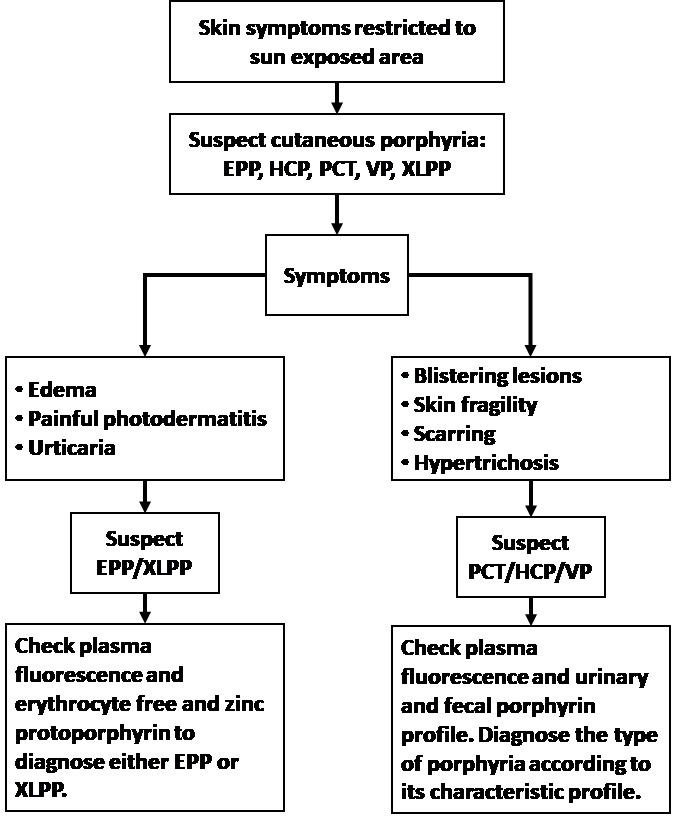
The porphyrias are a group of rare metabolic disorders, inherited or acquired, along the heme biosynthetic pathway, which could manifest with neurovisceral and/or cutaneous symptoms, depending on the defective enzyme. Neurovisceral porphyrias are characterized by acute attacks, in which excessive heme production is induced following exposure to a trigger. An acute attack usually presents with severe abdominal pain, vomiting, and tachycardia. Other symptoms which could appear include hypertension, hyponatremia, peripheral neuropathy, and mild mental symptoms. In severe attacks there could be severe symptoms including seizures and psychosis. If untreated, the attack might become very severe, affecting the peripheral, central, and autonomic nervous system, leading to paralysis, respiratory failure, hyponatremia, coma, and even death. From the biochemical point of view, acute attacks are involved with increased levels of precursors in the heme biosynthetic pathway, up to the deficient step. Of these precursors, aminolevulinic acid (ALA) is considered to be neurotoxic. Treatment is directed to reduce ALA production by reducing the activity of the enzyme aminolevulinate synthase (ALAS)-most effectively by heme therapy. Cutaneous symptoms are a consequence of elevated porphyrins in the blood stream. These porphyrins react to light; therefore sun-exposed areas are affected, producing fragile erosive skin lesions in porphyria cutanea tarda (PCT) or non-scarring stinging and burning symptoms in erythropoietic protoporphyria (EPP). Unlike the most common neurovisceral porphyria, acute intermittent porphyria (AIP), variegate porphyria (VP), and hereditary coproporphyria (HCP) can have cutaneous symptoms as well. Differentiating them from other cutaneous porphyrias is essential for accurate diagnosis, treatment, and patient recommendations.
Conflict of interest statement
Figures
References
-
- Besur S, Schmeltzer P, Bonkovsky HL. Acute porphyrias. J Emerg Med. 2015;49:305–12. https://doi.org/10.1016/j.jemermed.2015.04.034. - DOI - PubMed
-
- Bissell DM, Anderson KE, Bonkovsky HL. Porphyria. N Engl J Med. 2017;377:862–72. https://doi.org/10.1056/NEJMra1608634. - DOI - PubMed
-
- Karim Z, Lyoumi S, Nicolas G, Deybach JC, Gouya L, Puy H. Porphyrias: a 2015 update. Clin Res Hepatol Gastroenterol. 2015;39:412–25. https://doi.org/10.1016/j.clinre.2015.05.009. - DOI - PubMed
-
- Bissell DM, Lai JC, Meister RK, Blanc PD. Role of delta-aminolevulinic acid in the symptoms of acute porphyria. Am J Med. 2015;128:313–17. https://doi.org/10.1016/j.amjmed.2014.10.026. - DOI - PMC - PubMed
-
- Meyer UA, Schuurmans MM, Lindberg RL. Acute porphyrias: pathogenesis of neurological manifestations. Semin Liver Dis. 1998;18:43–52. https://doi.org/10.1055/s-2007-1007139. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous