

Impaired Trunk Flexor Strength, Fatigability, and Steadiness in Postpartum Women
- PMID: 29554014
- PMCID: PMC6045430
- DOI: 10.1249/MSS.0000000000001609
Impaired Trunk Flexor Strength, Fatigability, and Steadiness in Postpartum Women
Abstract
Purpose: To determine whether postpartum women (vaginal and cesarean delivery) have deficits in trunk flexor strength, fatigability and steadiness, compared with nulligravid women, up to 26 wk postpartum. We hypothesized that postpartum women would be weaker, more fatigable, and have greater torque fluctuations than controls, with cesarean delivery showing greater deficits than vaginal delivery.
Methods: Twenty-two control women (nulligravid) and 29 postpartum women (20-40 yr, 19 who delivered via vaginal birth, 13 via Caesarian section) participated. Postpartum women were tested 8 to 10 wk and 24 to 26 wk postpartum. Control women were tested 16 to 18 wk apart. Maximal voluntary isometric contractions (MVC) were performed at multiple trunk positions with the trunk flexor muscles. To determine trunk flexor fatigability, subjects performed intermittent isometric contractions at 50% MVC (6-s contraction, 4-s rest) in upright sitting until task failure. An MVC was performed during the fatiguing task (one per minute) and at 10 and 20 min of recovery.
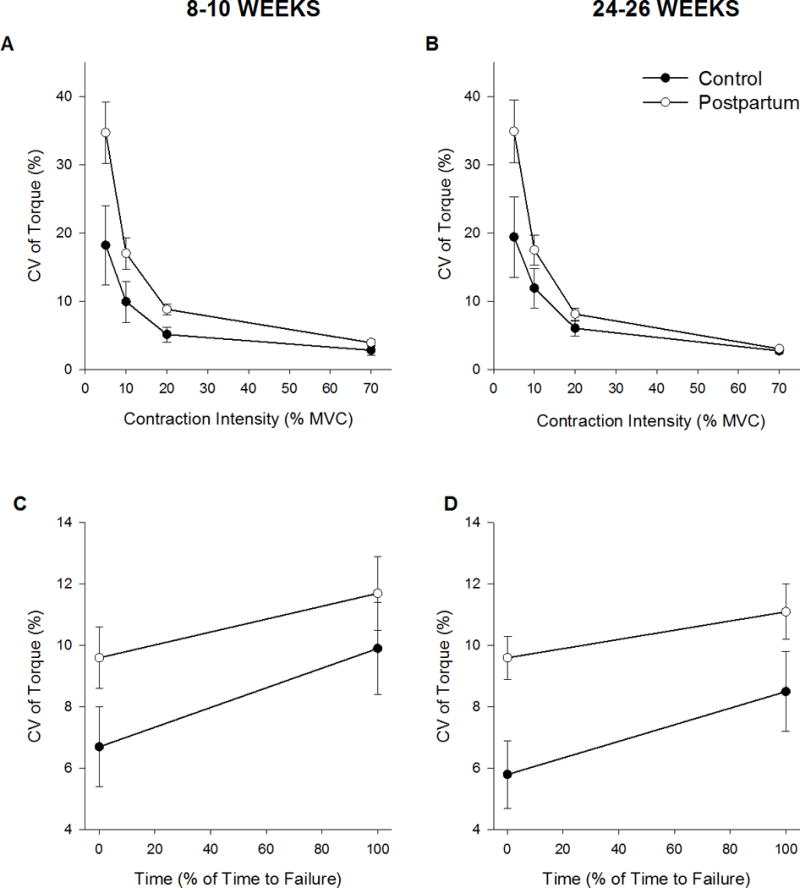
Results: At 8 and 26 wk, postpartum women (groups pooled) were weaker at all trunk angles (38% and 44% respectively, P < 0.05) than controls despite no differences in handgrip strength. Postpartum women were more fatigable (71% and 52% respectively) and had greater torque fluctuations than controls (P < 0.05). At 8 wk postpartum, women who had a cesarean delivery, were 59% more fatigable (P = 0.004) than the vaginal delivery group, with no difference between delivery types at 26 wk postpartum.
Conclusions: Musculoskeletal recovery, including trunk flexor muscle strength and fatigability, is incomplete at 26 wk postpartum. These findings provide a rationale for future studies to address outcomes of rehabilitation programs specifically targeted at improving strength and fatigability of the trunk flexor muscles after pregnancy and childbirth.
Conflict of interest statement
The authors report no conflicts of interest. The results of this study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. The results of this study do not constitute endorsement by ACSM, are solely the responsibility of the authors, and do not necessarily represent the official views of the NIH.
Figures


Similar articles
-
Muscle function and fatigability of trunk flexors in males and females.Biol Sex Differ. 2017 Apr 17;8:12. doi: 10.1186/s13293-017-0133-y. eCollection 2017. Biol Sex Differ. 2017. PMID: 28428836 Free PMC article.
-
Fatiguing handgrip exercise alters maximal force-generating capacity of plantar-flexors.Eur J Appl Physiol. 2013 Mar;113(3):559-66. doi: 10.1007/s00421-012-2462-1. Epub 2012 Jul 26. Eur J Appl Physiol. 2013. PMID: 22833010 Clinical Trial.
-
Sex differences in fatigability and recovery relative to the intensity-duration relationship.J Physiol. 2019 Dec;597(23):5577-5595. doi: 10.1113/JP278699. Epub 2019 Oct 30. J Physiol. 2019. PMID: 31529693
-
Men are more fatigable than strength-matched women when performing intermittent submaximal contractions.J Appl Physiol (1985). 2004 Jun;96(6):2125-32. doi: 10.1152/japplphysiol.01342.2003. Epub 2004 Feb 13. J Appl Physiol (1985). 2004. PMID: 14966025
-
Sex differences in fatigability of dynamic contractions.Exp Physiol. 2016 Feb;101(2):250-5. doi: 10.1113/EP085370. Epub 2015 Nov 17. Exp Physiol. 2016. PMID: 26440505 Free PMC article. Review.
Cited by
-
Do Measures of Muscular Fitness Modify the Effect of Intra-abdominal Pressure on Pelvic Floor Support in Postpartum Women?Female Pelvic Med Reconstr Surg. 2021 Feb 1;27(2):e267-e276. doi: 10.1097/SPV.0000000000000901. Female Pelvic Med Reconstr Surg. 2021. PMID: 32657824 Free PMC article.
-
New Assessment Tool-Postpartum Functional Assessment Questionnaire.Medicina (Kaunas). 2023 Jun 29;59(7):1219. doi: 10.3390/medicina59071219. Medicina (Kaunas). 2023. PMID: 37512032 Free PMC article.
-
Prioritise safety, optimise success! Return to rugby postpartum.Eur J Sport Sci. 2024 Dec;24(12):1701-1718. doi: 10.1002/ejsc.12144. Epub 2024 Jul 8. Eur J Sport Sci. 2024. PMID: 38978338 Free PMC article. Review.
-
Physical activity in the early postpartum period in primiparous women.J Sci Med Sport. 2021 Nov;24(11):1149-1154. doi: 10.1016/j.jsams.2021.06.009. Epub 2021 Jun 21. J Sci Med Sport. 2021. PMID: 34244085 Free PMC article.
-
Fatigability of the Lumbopelvic Stabilizing Muscles in Women 8 and 26 Weeks Postpartum.J Womens Health Phys Therap. 2018 Sep-Dec;42(3):128-138. doi: 10.1097/JWH.0000000000000109. J Womens Health Phys Therap. 2018. PMID: 30740039 Free PMC article.
References
-
- Boissonnault JS, Blaschak MJ. Incidence of Diastasis Recti Abdominis during the Childbearing Year. Physical Therapy. 1988;68(7):1082–6. - PubMed
-
- Kristiansson P, Svardsudd K, von Schoultz B. Reproductive hormones and aminoterminal propeptide of type III procollagen in serum as early markers of pelvic pain during late pregnancy. American Journal of Obstetrics and Gynecology. 1999;180(1):128–34. - PubMed
-
- Neumann DA. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. Third. St Louis, MO: Mosby Elsevier; 2016.
-
- Hodges PW, Kaigle Holm A, Holm S, Ekström L, Cresswell A, Hansson T, et al. Intervertebral stiffness of the spine is increased by evoked contraction of transversus abdominis and the diaphragm: in vivo porcine studies. Spine (Phila Pa 1976) 2003;28(23):2594–601. doi: 10.1097/01.BRS.0000096676.14323.25. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
