

Influence of model assumptions about HIV disease progression after initiating or stopping treatment on estimates of infections and deaths averted by scaling up antiretroviral therapy
- PMID: 29554136
- PMCID: PMC5858778
- DOI: 10.1371/journal.pone.0194220
Influence of model assumptions about HIV disease progression after initiating or stopping treatment on estimates of infections and deaths averted by scaling up antiretroviral therapy
Abstract
Background: Many mathematical models have investigated the population-level impact of expanding antiretroviral therapy (ART), using different assumptions about HIV disease progression on ART and among ART dropouts. We evaluated the influence of these assumptions on model projections of the number of infections and deaths prevented by expanded ART.
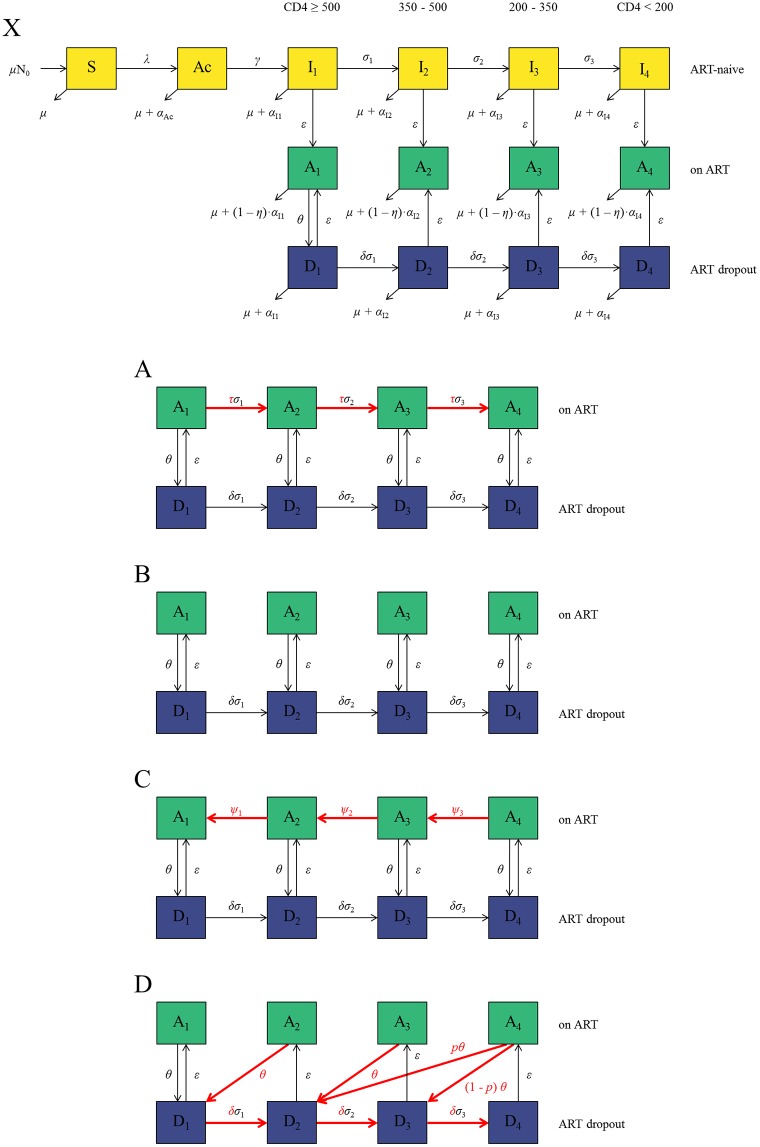
Methods: A new dynamic model of HIV transmission among men who have sex with men (MSM) was developed, which incorporated each of four alternative assumptions about disease progression used in previous models: (A) ART slows disease progression; (B) ART halts disease progression; (C) ART reverses disease progression by increasing CD4 count; (D) ART reverses disease progression, but disease progresses rapidly once treatment is stopped. The model was independently calibrated to HIV prevalence and ART coverage data from the United States under each progression assumption in turn. New HIV infections and HIV-related deaths averted over 10 years were compared for fixed ART coverage increases.
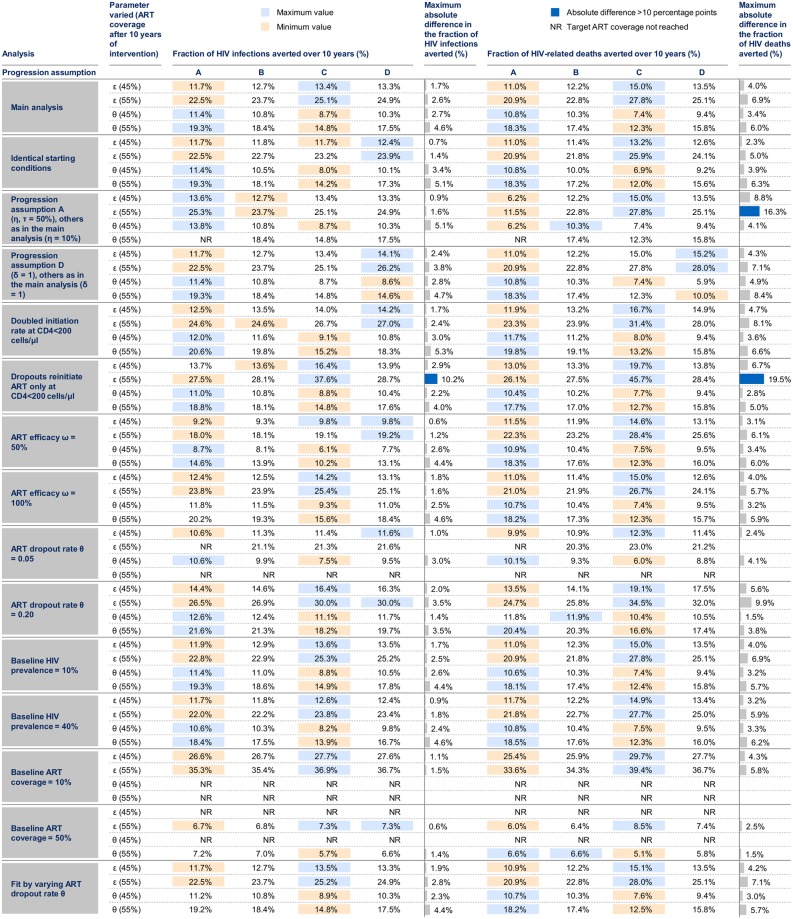
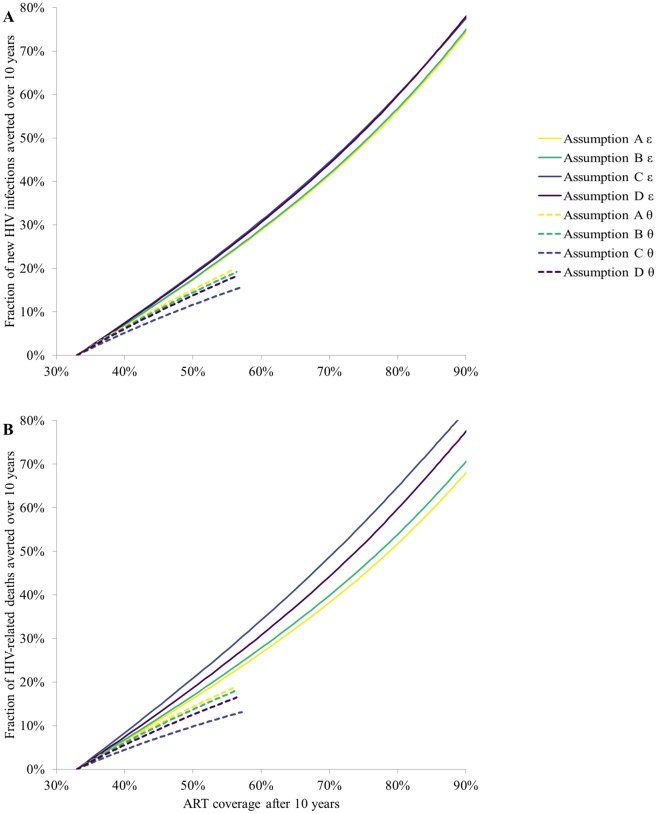
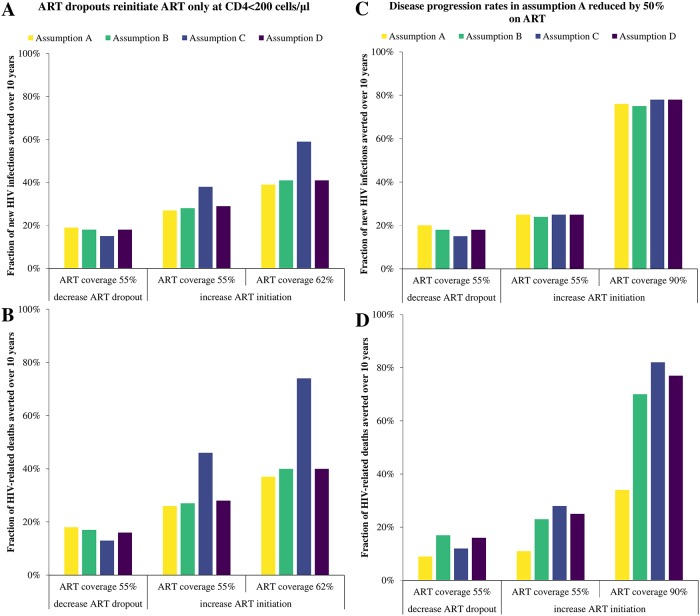
Results: Little absolute difference (<7 percentage points (pp)) in HIV infections averted over 10 years was seen between progression assumptions for the same increases in ART coverage (varied between 33% and 90%) if ART dropouts reinitiated ART at the same rate as ART-naïve MSM. Larger differences in the predicted fraction of HIV-related deaths averted were observed (up to 15pp). However, if ART dropouts could only reinitiate ART at CD4<200 cells/μl, assumption C predicted substantially larger fractions of HIV infections and deaths averted than other assumptions (up to 20pp and 37pp larger, respectively).
Conclusion: Different disease progression assumptions on and post-ART interruption did not affect the fraction of HIV infections averted with expanded ART, unless ART dropouts only re-initiated ART at low CD4 counts. Different disease progression assumptions had a larger influence on the fraction of HIV-related deaths averted with expanded ART.
Conflict of interest statement
Figures
References
-
- Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, Van Lunzen J, et al. Sexual activity without condoms and risk of hiv transmission in serodifferent couples when the hiv-positive partner is using suppressive antiretroviral therapy. The Journal of the American Medical Association. 2016;316(2):171–81. 10.1001/jama.2016.5148 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
