

Association of Hypercapnia and Hypercapnic Acidosis With Clinical Outcomes in Mechanically Ventilated Patients With Cerebral Injury
- PMID: 29554187
- PMCID: PMC5885161
- DOI: 10.1001/jamaneurol.2018.0123
Association of Hypercapnia and Hypercapnic Acidosis With Clinical Outcomes in Mechanically Ventilated Patients With Cerebral Injury
Abstract
Importance: Clinical studies investigating the effects of hypercapnia and hypercapnic acidosis in acute cerebral injury are limited. The studies performed so far have mainly focused on the outcomes in relation to the changes in partial pressure of carbon dioxide and pH in isolation and have not evaluated the effects of partial pressure of carbon dioxide and pH in conjunction.
Objective: To review the association of compensated hypercapnia and hypercapnic acidosis during the first 24 hours of intensive care unit admission on hospital mortality in adult mechanically ventilated patients with cerebral injury.
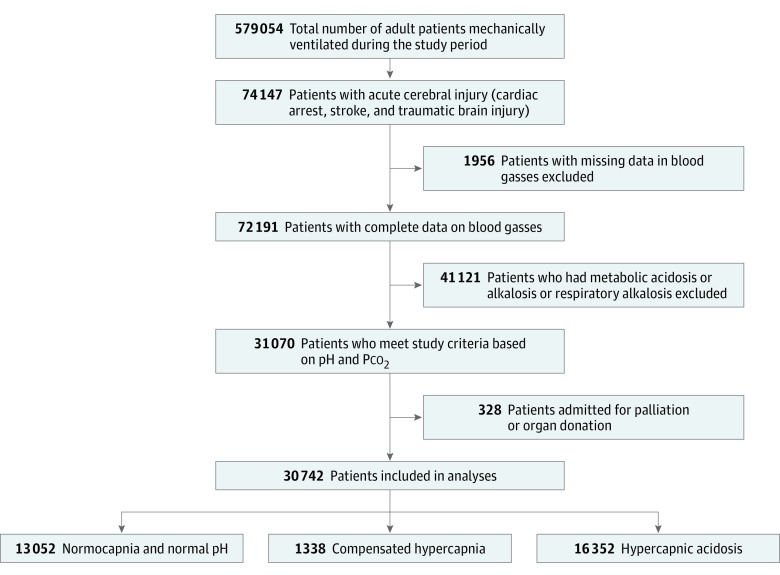
Design, setting, and participants: Multicenter, binational retrospective review of patients with cerebral injury (traumatic brain injury, cardiac arrest, and stroke) admitted to 167 intensive care units in Australia and New Zealand between January 2000 and December 2015. Patients were classified into 3 groups based on combination of arterial pH and arterial carbon dioxide (normocapnia and normal pH, compensated hypercapnia, and hypercapnic acidosis) during the first 24 hours of intensive care unit stay.
Main outcomes and measures: Hospital mortality.
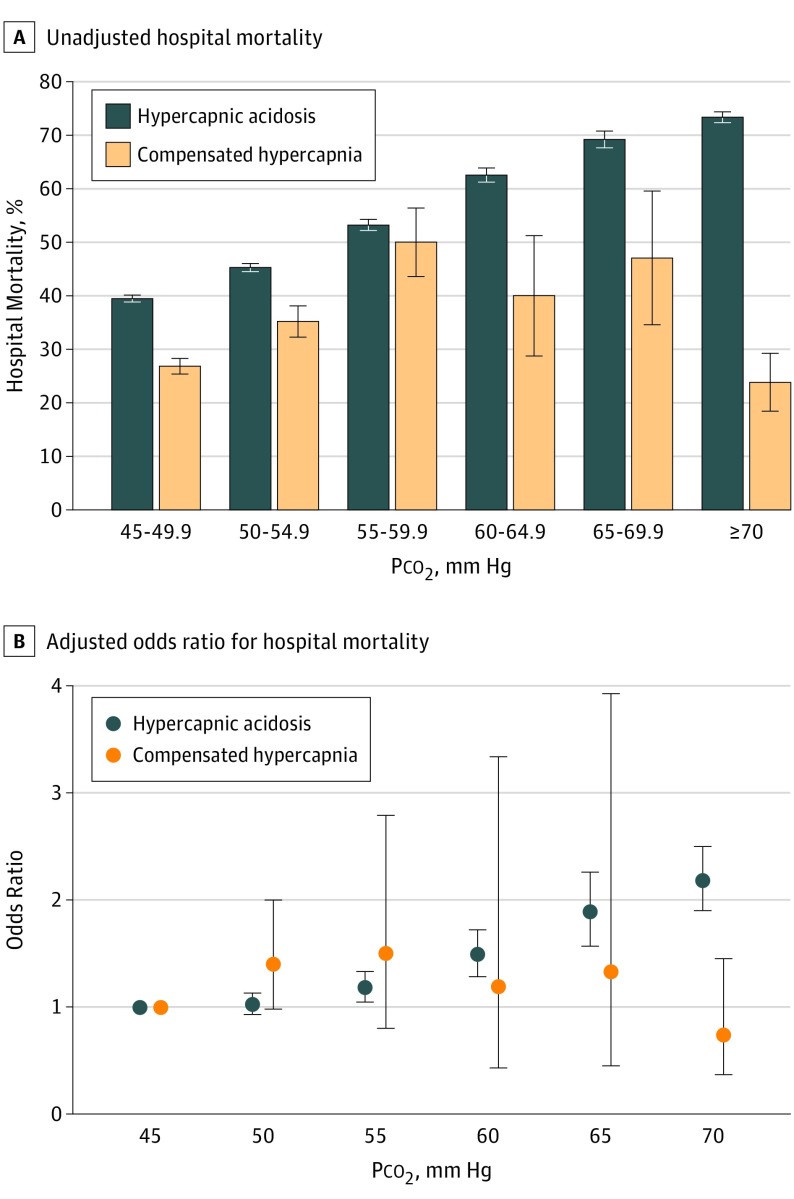
Results: A total of 30 742 patients (mean age, 55 years; 21 827 men [71%]) were included. Unadjusted hospital mortality rates were highest in patients with hypercapnic acidosis. Multivariable logistic regression analysis and Cox proportional hazards analysis in 3 diagnostic categories showed increased odds of hospital mortality (cardiac arrest odds ratio [OR], 1.51; 95% CI, 1.34-1.71; stroke OR, 1.43; 95% CI, 1.27-1.6; and traumatic brain injury OR, 1.22; 95% CI, 1.06-1.42; P <.001) and hazard ratios (HR) (cardiac arrest HR, 1.23; 95% CI, 1.14-1.34; stroke HR, 1.3; 95% CI, 1.21-1.4; traumatic brain injury HR, 1.13; 95% CI, 1-1.27), in patients with hypercapnic acidosis compared with normocapnia and normal pH. There was no difference in mortality between patients who had compensated hypercapnia compared with patients who had normocapnia and normal pH. In patients with hypercapnic acidosis, the adjusted OR of hospital mortality increased with increasing partial pressure of carbon dioxide, while no such increase was noted in patients with compensated hypercapnia.
Conclusions and relevance: Hypercapnic acidosis was associated with increased risk of hospital mortality in patients with cerebral injury. Hypercapnia, when compensated to normal pH during the first 24 hours of intensive care unit admission, may not be harmful in mechanically ventilated patients with cerebral injury.
Conflict of interest statement
Figures
Comment in
-
Arterial Partial Pressure of Carbon Dioxide and Secondary Brain Injury-6 Degrees of Separation?JAMA Neurol. 2018 Jul 1;75(7):787-788. doi: 10.1001/jamaneurol.2018.0003. JAMA Neurol. 2018. PMID: 29554181 No abstract available.
-
What Is the Association With Dissociation?JAMA Neurol. 2018 Dec 1;75(12):1571-1572. doi: 10.1001/jamaneurol.2018.3220. JAMA Neurol. 2018. PMID: 30383095 No abstract available.
-
What is the Association With Dissociation?-Reply.JAMA Neurol. 2018 Dec 1;75(12):1572-1573. doi: 10.1001/jamaneurol.2018.3237. JAMA Neurol. 2018. PMID: 30383101 No abstract available.
References
-
- Maas AI, Dearden M, Teasdale GM, et al. ; European Brain Injury Consortium . EBIC-guidelines for management of severe head injury in adults. Acta Neurochir (Wien). 1997;139(4):286-294. - PubMed
-
- Davis DP, Idris AH, Sise MJ, et al. Early ventilation and outcome in patients with moderate to severe traumatic brain injury. Crit Care Med. 2006;34(4):1202-1208. - PubMed
-
- Roberts BW, Kilgannon JH, Chansky ME, Mittal N, Wooden J, Trzeciak S. Association between postresuscitation partial pressure of arterial carbon dioxide and neurological outcome in patients with post-cardiac arrest syndrome. Circulation. 2013;127(21):2107-2113. - PubMed
-
- Schneider AG, Eastwood GM, Bellomo R, et al. Arterial carbon dioxide tension and outcome in patients admitted to the intensive care unit after cardiac arrest. Resuscitation. 2013;84(7):927-934. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
