

Effects of Celecoxib and Low-dose Aspirin on Outcomes in Adjuvant Aromatase Inhibitor-Treated Patients: CCTG MA.27
- PMID: 29554282
- PMCID: PMC6669949
- DOI: 10.1093/jnci/djy017
Effects of Celecoxib and Low-dose Aspirin on Outcomes in Adjuvant Aromatase Inhibitor-Treated Patients: CCTG MA.27
Abstract
Background: Celecoxib and low-dose aspirin might decrease risk of breast cancer recurrence.
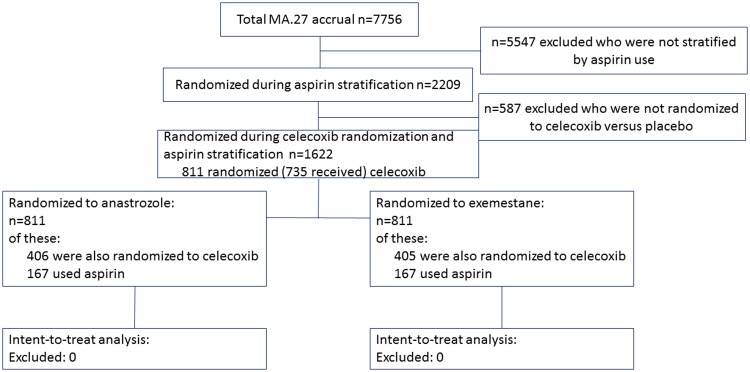
Methods: In the Canadian Cancer Trials Group MA.27, postmenopausal hormone receptor-positive breast cancer patients were randomly assigned (2 × 2) to adjuvant exemestane or anastrozole, and celecoxib or placebo. Low-dose aspirin of 81 mg or less was a stratification factor. Due to concerns about cardiac toxicity, celecoxib use was stopped in December 2004, while stratification by aspirin use was removed through protocol amendment. We examined the effects of celecoxib and low-dose aspirin on event-free survival (EFS), defined as time from random assignment to time of locoregional or distant disease recurrence, new primary breast cancer, or death from any cause; distant disease-free survival (DDFS); and overall survival (OS). All statistical tests were two-sided.
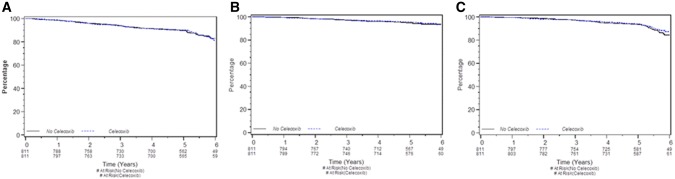
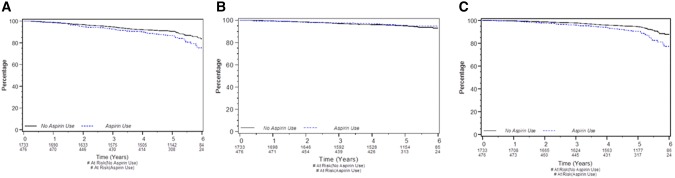
Results: Random assignment to celecoxib (n = 811, 50.0%) or placebo (n = 811, 50.0%) was discontinued after 18 months (n = 1622). At a median of 4.1 years' follow-up, among 1622 patients, 186 (11.5%) patients had an EFS event: 80 (4.9%) had distant relapse, and 125 (7.7%) died from any cause. Celecoxib did not statistically significantly impact EFS, DDFS, or OS in univariate analysis (respectively, P = .92, P = .55, and P = .56) or multivariable analysis (respectively, P = .74, P = .60, and P = .76). Low-dose aspirin use (aspirin users n = 476, 21.5%; non-aspirin users n = 1733, 78.5%) was associated in univariate analyses with worse EFS (hazard ratio [HR] = 1.48, 95% confidence interval [CI] = 1.12 to 1.96, P = 0.006) and worse OS (HR = 1.87, 95% CI = 1.35 to 2.61, P < .001). After adjusting for baseline characteristics and treatment arm, aspirin use showed no statistical association with EFS (P = .08) and DDFS (P = .82), but was associated with statistically worse OS (HR = 1.67, 95% CI = 1.13 to 2.49, P = .01).
Conclusion: Random assignment to short-term (≤18 months) celecoxib as well as use of low-dose aspirin showed no effect on DDFS and EFS in multivariable analysis. Low-dose aspirin increased "all-cause" mortality, presumably because of higher preexisting cardiovascular risks.
Trial registration: ClinicalTrials.gov NCT00066573.
Figures
Comment in
-
NSAIDs to Prevent Breast Cancer Recurrence? An Unanswered Question.J Natl Cancer Inst. 2018 Sep 1;110(9):927-928. doi: 10.1093/jnci/djy049. J Natl Cancer Inst. 2018. PMID: 29554350 Free PMC article. No abstract available.
References
-
- Half E, Tang XM, Gwyn K, et al. Cyclooxygenase-2 expression in human breast cancers and adjacent ductal carcinoma in situ. Cancer Res. 2002;626:1676–1681. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
