

Serum potassium and adverse outcomes across the range of kidney function: a CKD Prognosis Consortium meta-analysis
- PMID: 29554312
- PMCID: PMC5930249
- DOI: 10.1093/eurheartj/ehy100
Serum potassium and adverse outcomes across the range of kidney function: a CKD Prognosis Consortium meta-analysis
Abstract
Aims: Both hypo- and hyperkalaemia can have immediate deleterious physiological effects, and less is known about long-term risks. The objective was to determine the risks of all-cause mortality, cardiovascular mortality, and end-stage renal disease associated with potassium levels across the range of kidney function and evaluate for consistency across cohorts in a global consortium.
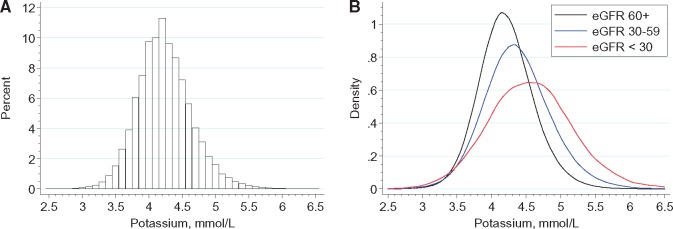
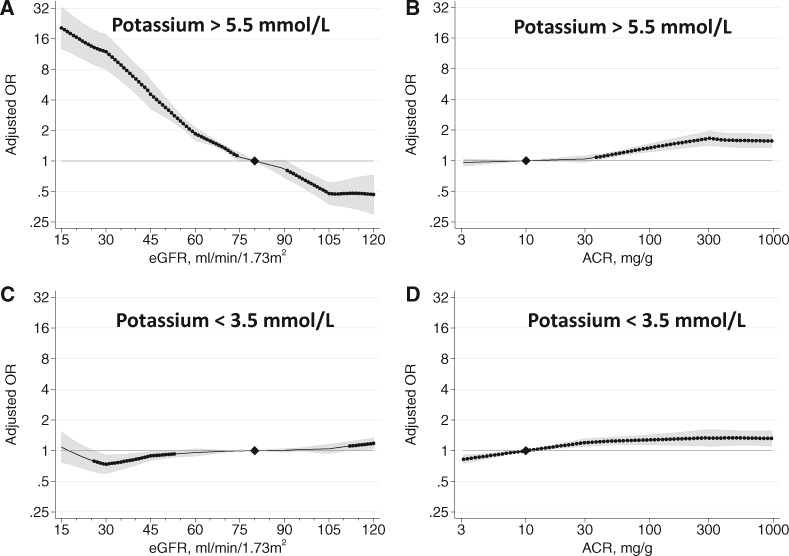
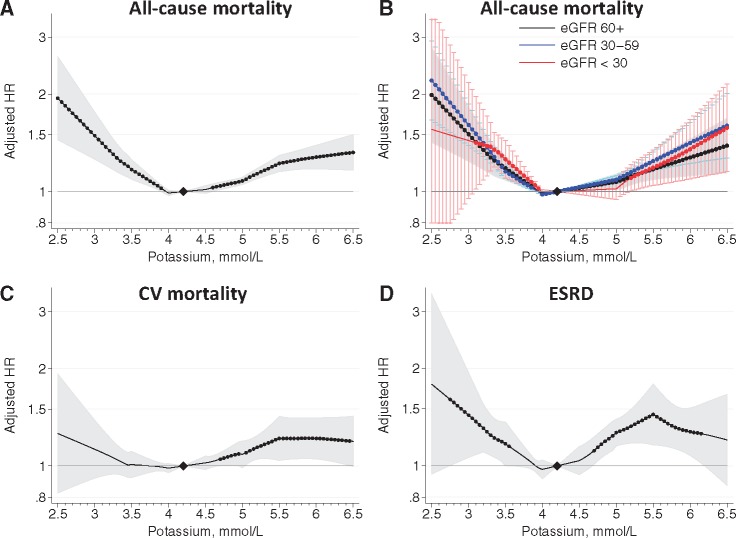
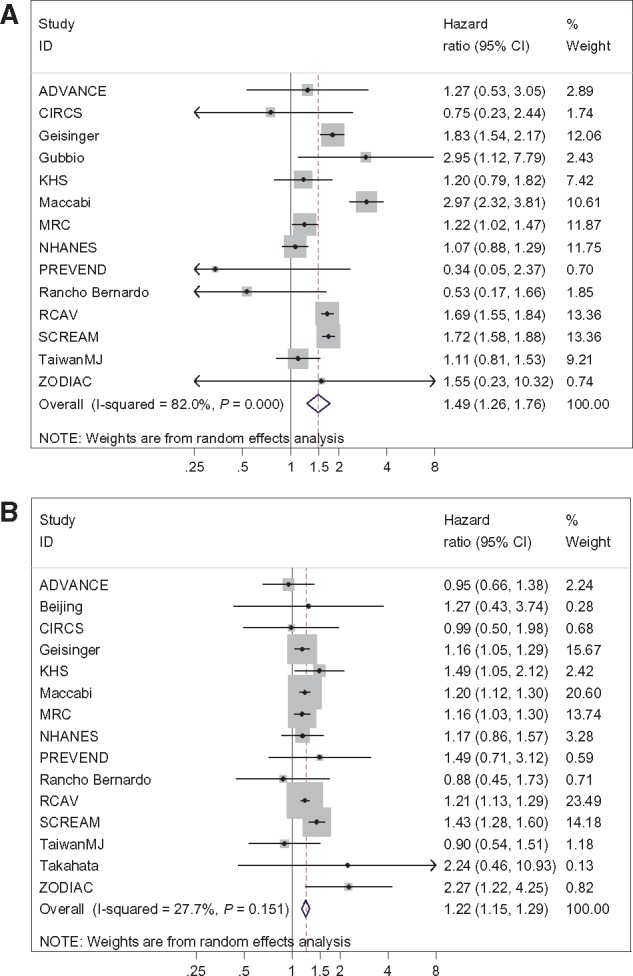
Methods and results: We performed an individual-level data meta-analysis of 27 international cohorts [10 general population, 7 high cardiovascular risk, and 10 chronic kidney disease (CKD)] in the CKD Prognosis Consortium. We used Cox regression followed by random-effects meta-analysis to assess the relationship between baseline potassium and adverse outcomes, adjusted for demographic and clinical characteristics, overall and across strata of estimated glomerular filtration rate (eGFR) and albuminuria. We included 1 217 986 participants followed up for a mean of 6.9 years. The average age was 55 ± 16 years, average eGFR was 83 ± 23 mL/min/1.73 m2, and 17% had moderate- to-severe increased albuminuria levels. The mean baseline potassium was 4.2 ± 0.4 mmol/L. The risk of serum potassium of >5.5 mmol/L was related to lower eGFR and higher albuminuria. The risk relationship between potassium levels and adverse outcomes was U-shaped, with the lowest risk at serum potassium of 4-4.5 mmol/L. Compared with a reference of 4.2 mmol/L, the adjusted hazard ratio for all-cause mortality was 1.22 [95% confidence interval (CI) 1.15-1.29] at 5.5 mmol/L and 1.49 (95% CI 1.26-1.76) at 3.0 mmol/L. Risks were similar by eGFR, albuminuria, renin-angiotensin-aldosterone system inhibitor use, and across cohorts.
Conclusions: Outpatient potassium levels both above and below the normal range are consistently associated with adverse outcomes, with similar risk relationships across eGFR and albuminuria.
Figures
Comment in
-
Potassium: an ion with dangerous airs and graces.Eur Heart J. 2018 May 1;39(17):1543-1545. doi: 10.1093/eurheartj/ehy159. Eur Heart J. 2018. PMID: 29579264
References
-
- Dittrich KL, Walls RM.. Hyperkalemia: eCG manifestations and clinical considerations. J Emerg Med 1986;4:449–455. - PubMed
-
- Priori SG, Blomstrom-Lundqvist C.. 2015 European Society of Cardiology Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death summarized by co-chairs. Eur Heart J 2015;36:2757–2759. - PubMed
-
- Bourgoignie JJ, Kaplan M, Pincus J, Gavellas G, Rabinovitch A.. Renal handling of potassium in dogs with chronic renal insufficiency. Kidney Int 1981;20:482–490. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
