

Estimating Breast Cancer Survival by Molecular Subtype in the Absence of Screening and Adjuvant Treatment
- PMID: 29554464
- PMCID: PMC6635303
- DOI: 10.1177/0272989X17743236
Estimating Breast Cancer Survival by Molecular Subtype in the Absence of Screening and Adjuvant Treatment
Abstract
Background: As molecular subtyping of breast cancer influences clinical management, the evaluation of screening and adjuvant treatment interventions at the population level needs to account for molecular subtyping. Performing such analyses are challenging because molecular subtype-specific, long-term outcomes are not readily accessible; these markers were not historically recorded in tumor registries. We present a modeling approach to estimate historical survival outcomes by estrogen receptor (ER) and human epidermal growth factor receptor 2 (HER2) status.
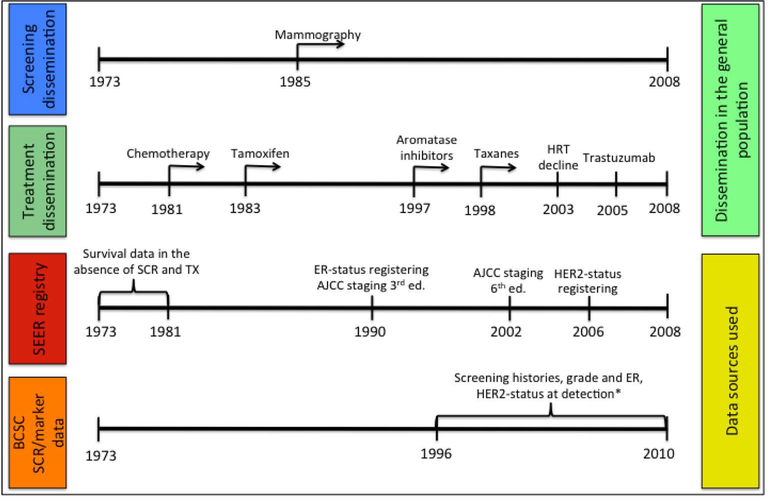
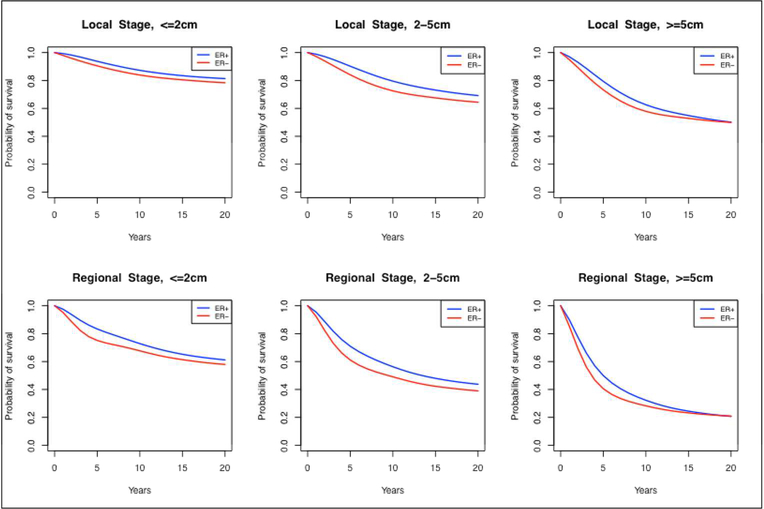
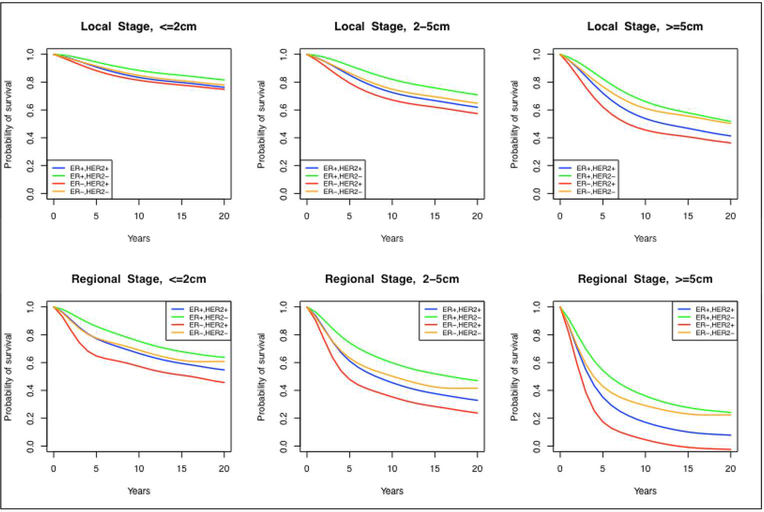
Method: Our approach leverages a simulation model of breast cancer outcomes and integrates data from two sources: the Surveillance Epidemiology and End Results (SEER) databases and the Breast Cancer Surveillance Consortium (BCSC). We not only produce ER- and HER2-specific estimates of breast cancer survival in the absence of screening and adjuvant treatment but we also estimate mean tumor volume doubling time (TVDT) and mean mammographic detection threshold by ER/HER2-status.
Results: In general, we found that tumors with ER-negative and HER2-positive status are associated with more aggressive growth, have lower TVDTs, are harder to detect by mammography, and have worse survival outcomes in the absence of screening and adjuvant treatment. Our estimates have been used as inputs into model-based analyses that evaluate the effects of screening and adjuvant treatment interventions on population outcomes by ER and HER2 status developed by the Cancer Intervention and Surveillance Modeling Network (CISNET) Breast Cancer Working Group. In addition, our estimates enable a re-assessment of historical trends in breast cancer incidence and mortality in terms of contemporary molecular tumor characteristics.
Conclusion: Our approach can be generalized beyond breast cancer and to more complex molecular profiles.
Keywords: CISNET; breast cancer simulation model; breast cancer survival; estrogen receptor (ER) status; human epidermal growth factor 2 (HER2) status; screening mammography.
Figures
Similar articles
-
A Molecular Subtype-Specific Stochastic Simulation Model of US Breast Cancer Incidence, Survival, and Mortality Trends from 1975 to 2010.Med Decis Making. 2018 Apr;38(1_suppl):89S-98S. doi: 10.1177/0272989X17737508. Med Decis Making. 2018. PMID: 29554473 Free PMC article.
-
Mathematical Modeling to Address Questions in Breast Cancer Screening: An Overview of the Breast Cancer Models of the Cancer Intervention and Surveillance Modeling Network.J Breast Imaging. 2025 Mar 18;7(2):141-154. doi: 10.1093/jbi/wbaf003. J Breast Imaging. 2025. PMID: 40036318 Review.
-
Association of Screening and Treatment With Breast Cancer Mortality by Molecular Subtype in US Women, 2000-2012.JAMA. 2018 Jan 9;319(2):154-164. doi: 10.1001/jama.2017.19130. JAMA. 2018. PMID: 29318276 Free PMC article.
-
Effects of screening and systemic adjuvant therapy on ER-specific US breast cancer mortality.J Natl Cancer Inst. 2014 Sep 24;106(11):dju289. doi: 10.1093/jnci/dju289. Print 2014 Nov. J Natl Cancer Inst. 2014. PMID: 25255803 Free PMC article.
-
A Review of Biosensors for Detecting Tumor Markers in Breast Cancer.Life (Basel). 2022 Feb 25;12(3):342. doi: 10.3390/life12030342. Life (Basel). 2022. PMID: 35330093 Free PMC article. Review.
Cited by
-
Common Model Inputs Used in CISNET Collaborative Breast Cancer Modeling.Med Decis Making. 2018 Apr;38(1_suppl):9S-23S. doi: 10.1177/0272989X17700624. Med Decis Making. 2018. PMID: 29554466 Free PMC article.
-
Cost-effectiveness of using artificial intelligence versus polygenic risk score to guide breast cancer screening.BMC Cancer. 2022 May 6;22(1):501. doi: 10.1186/s12885-022-09613-1. BMC Cancer. 2022. PMID: 35524200 Free PMC article.
-
A Molecular Subtype-Specific Stochastic Simulation Model of US Breast Cancer Incidence, Survival, and Mortality Trends from 1975 to 2010.Med Decis Making. 2018 Apr;38(1_suppl):89S-98S. doi: 10.1177/0272989X17737508. Med Decis Making. 2018. PMID: 29554473 Free PMC article.
-
Adjuvant Chemotherapy for Older Patients With Breast Cancer: When Is the Pain Worth the Gain?J Natl Cancer Inst. 2020 Jun 1;112(6):551-552. doi: 10.1093/jnci/djz192. J Natl Cancer Inst. 2020. PMID: 31612212 Free PMC article. No abstract available.
-
Mathematical Modeling to Address Questions in Breast Cancer Screening: An Overview of the Breast Cancer Models of the Cancer Intervention and Surveillance Modeling Network.J Breast Imaging. 2025 Mar 18;7(2):141-154. doi: 10.1093/jbi/wbaf003. J Breast Imaging. 2025. PMID: 40036318 Review.
References
-
- Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687–717. - PubMed
-
- Henson DE, Ries L, Freedman LS, Carriaga M. Relationship among outcome, stage of disease, and histologic grade for 22,616 cases of breast cancer. The basis for a prognostic index. Cancer. 1991;68(10):2142–9. - PubMed
-
- Kurian AW, Carlson RW. Chapter 17: Principles of Breast Cancer Therapy In: Li CI, ed. Breast Cancer Epidemiology: Springer; 2010:371–88.
-
- Vo T, Xing Y, Meric-Bernstam F, Mirza N, Vlastos G, Symmans WF, et al. Long-term outcomes in patients with mucinous, medullary, tubular, and invasive ductal carcinomas after lumpectomy. Am J Surg. 2007;194(4):527–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
