

Common Model Inputs Used in CISNET Collaborative Breast Cancer Modeling
- PMID: 29554466
- PMCID: PMC5862072
- DOI: 10.1177/0272989X17700624
Common Model Inputs Used in CISNET Collaborative Breast Cancer Modeling
Abstract
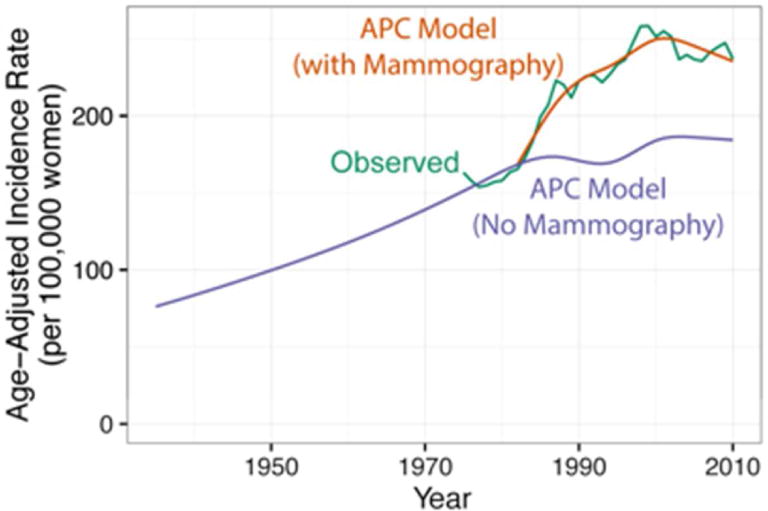
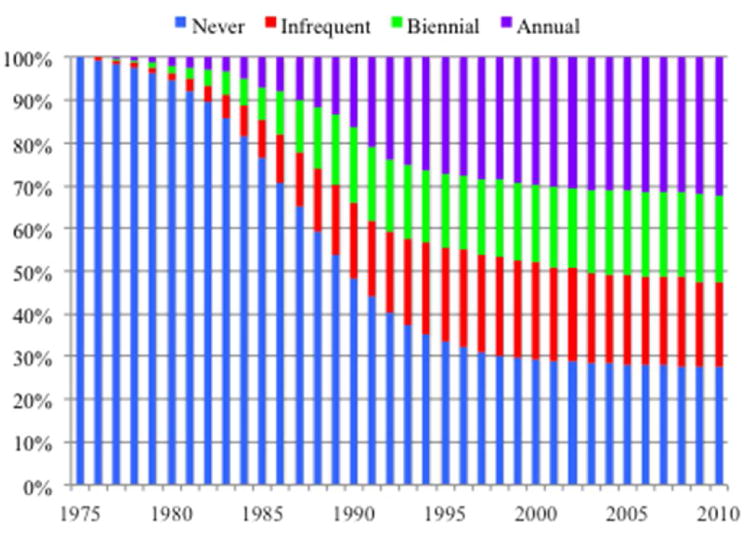
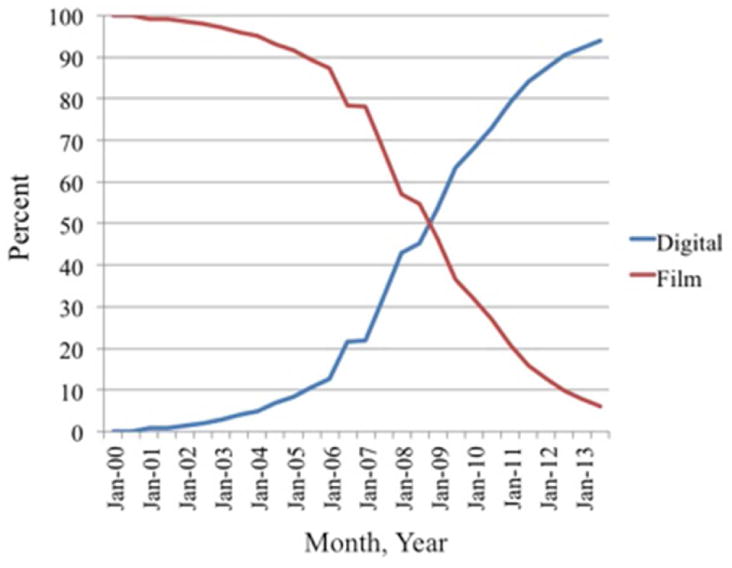
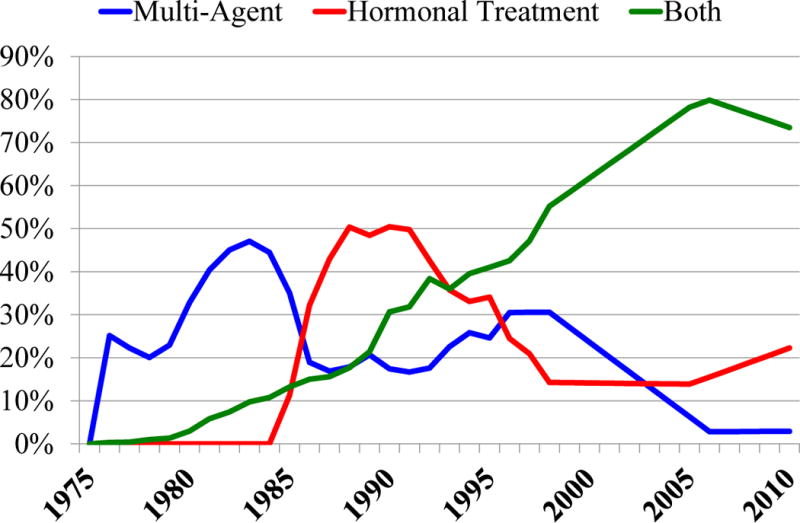
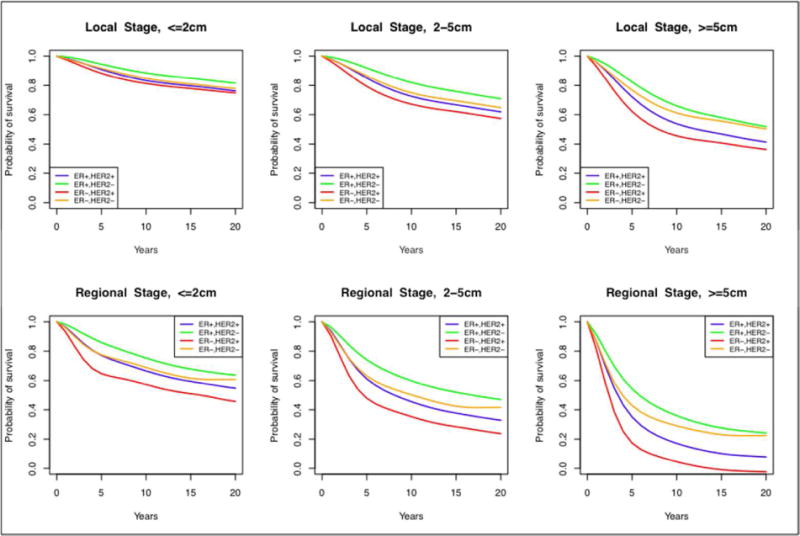
Background: Since their inception in 2000, the Cancer Intervention and Surveillance Network (CISNET) breast cancer models have collaborated to use a nationally representative core of common input parameters to represent key components of breast cancer control in each model. Employment of common inputs permits greater ability to compare model output than when each model begins with different input parameters. The use of common inputs also enhances inferences about the results, and provides a range of reasonable results based on variations in model structure, assumptions, and methods of use of the input values. The common input data are updated for each analysis to ensure that they reflect the most current practice and knowledge about breast cancer. The common core of parameters includes population rates of births and deaths; age- and cohort-specific temporal rates of breast cancer incidence in the absence of screening and treatment; effects of risk factors on incidence trends; dissemination of plain film and digital mammography; screening test performance characteristics; stage or size distribution of screen-, interval-, and clinically- detected tumors by age; the joint distribution of ER/HER2 by age and stage; survival in the absence of screening and treatment by stage and molecular subtype; age-, stage-, and molecular subtype-specific therapy; dissemination and effectiveness of therapies over time; and competing non-breast cancer mortality.
Method and results: In this paper, we summarize the methods and results for the common input values presently used in the CISNET breast cancer models, note assumptions made because of unobservable phenomena and/or unavailable data, and highlight plans for the development of future parameters.
Conclusion: These data are intended to enhance the transparency of the breast CISNET models.
Keywords: breast cancer epidemiology; cancer simulation; simulation models.
Figures
Similar articles
-
Comparing CISNET Breast Cancer Models Using the Maximum Clinical Incidence Reduction Methodology.Med Decis Making. 2018 Apr;38(1_suppl):112S-125S. doi: 10.1177/0272989X17743244. Med Decis Making. 2018. PMID: 29554471 Free PMC article.
-
Comparing CISNET Breast Cancer Incidence and Mortality Predictions to Observed Clinical Trial Results of Mammography Screening from Ages 40 to 49.Med Decis Making. 2018 Apr;38(1_suppl):140S-150S. doi: 10.1177/0272989X17718168. Med Decis Making. 2018. PMID: 29554468 Free PMC article.
-
A Molecular Subtype-Specific Stochastic Simulation Model of US Breast Cancer Incidence, Survival, and Mortality Trends from 1975 to 2010.Med Decis Making. 2018 Apr;38(1_suppl):89S-98S. doi: 10.1177/0272989X17737508. Med Decis Making. 2018. PMID: 29554473 Free PMC article.
-
Reflecting on 20 years of breast cancer modeling in CISNET: Recommendations for future cancer systems modeling efforts.PLoS Comput Biol. 2021 Jun 17;17(6):e1009020. doi: 10.1371/journal.pcbi.1009020. eCollection 2021 Jun. PLoS Comput Biol. 2021. PMID: 34138842 Free PMC article. Review.
-
Additional common inputs for analyzing impact of adjuvant therapy and mammography on U.S. mortality.J Natl Cancer Inst Monogr. 2006;(36):26-9. doi: 10.1093/jncimonographs/lgj005. J Natl Cancer Inst Monogr. 2006. PMID: 17032891 Review.
Cited by
-
Modeling Ductal Carcinoma In Situ (DCIS): An Overview of CISNET Model Approaches.Med Decis Making. 2018 Apr;38(1_suppl):126S-139S. doi: 10.1177/0272989X17729358. Med Decis Making. 2018. PMID: 29554463 Free PMC article.
-
Comparing CISNET Breast Cancer Models Using the Maximum Clinical Incidence Reduction Methodology.Med Decis Making. 2018 Apr;38(1_suppl):112S-125S. doi: 10.1177/0272989X17743244. Med Decis Making. 2018. PMID: 29554471 Free PMC article.
-
Reassessing the Benefits and Harms of Risk-Reducing Medication Considering the Persistent Risk of Breast Cancer Mortality in Estrogen Receptor-Positive Breast Cancer.J Clin Oncol. 2023 Feb 1;41(4):859-870. doi: 10.1200/JCO.22.01342. Epub 2022 Dec 1. J Clin Oncol. 2023. PMID: 36455167 Free PMC article.
-
Identifying Equitable Screening Mammography Strategies for Black Women in the United States Using Simulation Modeling.Ann Intern Med. 2021 Dec;174(12):1637-1646. doi: 10.7326/M20-6506. Epub 2021 Oct 19. Ann Intern Med. 2021. PMID: 34662151 Free PMC article.
-
Personalizing Breast Cancer Screening Based on Polygenic Risk and Family History.J Natl Cancer Inst. 2021 Apr 6;113(4):434-442. doi: 10.1093/jnci/djaa127. J Natl Cancer Inst. 2021. PMID: 32853342 Free PMC article.
References
-
- Weigel AP, Liniger MA, Appenzeller C. Can multi-model combination really enhance the prediction skill of probabilistic ensemble forecasts? Quarterly Journal of the Royal Meteorological Society QJR. Meteorol Soc. 2008;134:241–260. doi: 10.1002/qj.210. Published online in Wiley InterScience ( www.interscience.wiley.com) - DOI
-
- Huang X, Li Y, Song J, Berry D. The MD Anderson CISNET model for estimating benefits of adjuvant therapy and screening mammography for breast cancer: an update. Medical Decision Making. 2016 Submitted.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
