

Accelerating Stroke Recovery: Body Structures and Functions, Activities, Participation, and Quality of Life Outcomes From a Large Rehabilitation Trial
- PMID: 29554849
- PMCID: PMC5863583
- DOI: 10.1177/1545968318760726
Accelerating Stroke Recovery: Body Structures and Functions, Activities, Participation, and Quality of Life Outcomes From a Large Rehabilitation Trial
Abstract
Background: Task-oriented therapies have been developed to address significant upper extremity disability that persists after stroke. Yet, the extent of and approach to rehabilitation and recovery remains unsatisfactory to many.
Objective: To compare a skill-directed investigational intervention with usual care treatment for body functions and structures, activities, participation, and quality of life outcomes.
Methods: On average, 46 days poststroke, 361 patients were randomized to 1 of 3 outpatient therapy groups: a patient-centered Accelerated Skill Acquisition Program (ASAP), dose-equivalent usual occupational therapy (DEUCC), or usual therapy (UCC). Outcomes were taken at baseline, posttreatment, 6 months, and 1 year after randomization. Longitudinal mixed effect models compared group differences in poststroke improvement during treatment and follow-up phases.
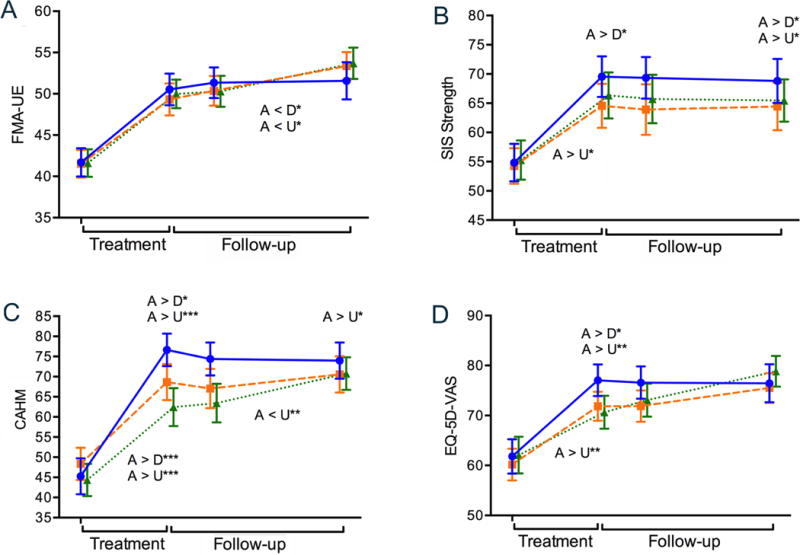
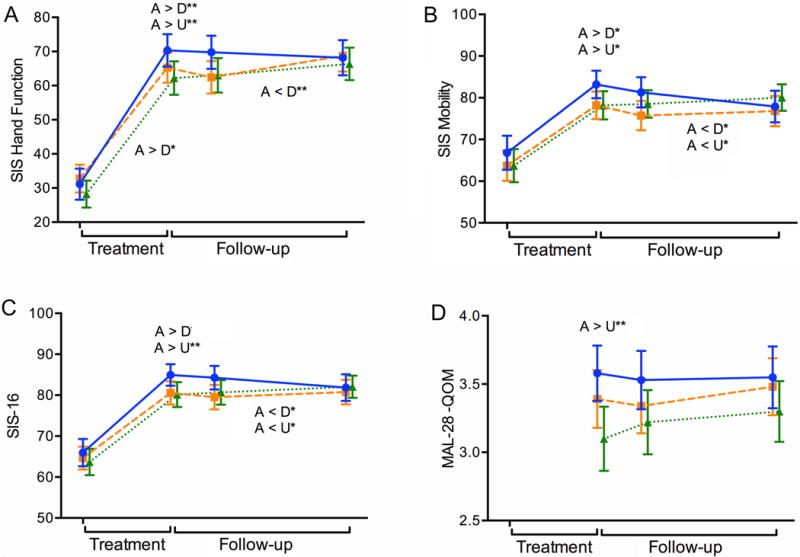
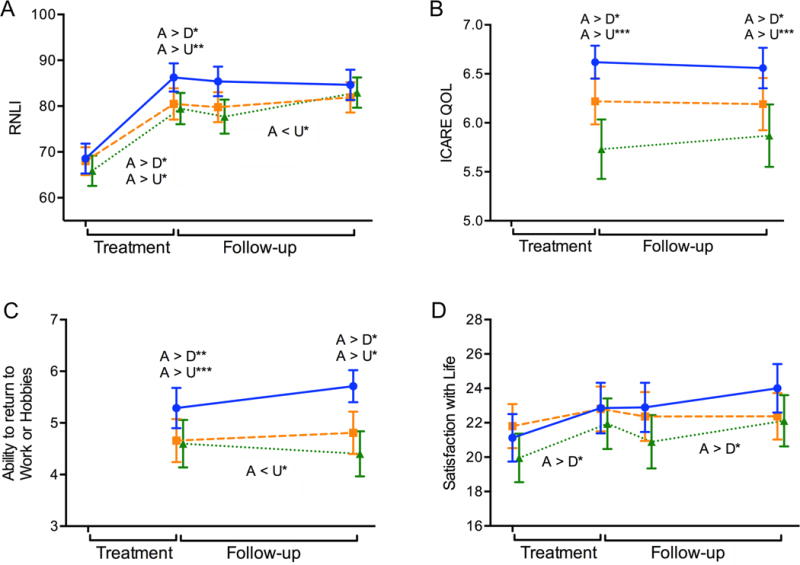
Results: Across all groups, most improvement occurred during the treatment phase, followed by change more slowly during follow-up. Compared with DEUCC and UCC, ASAP group gains were greater during treatment for Stroke Impact Scale Hand, Strength, Mobility, Physical Function, and Participation scores, self-efficacy, perceived health, reintegration, patient-centeredness, and quality of life outcomes. ASAP participants reported higher Motor Activity Log-28 Quality of Movement than UCC posttreatment and perceived greater study-related improvements in quality of life. By end of study, all groups reached similar levels with only limited group differences.
Conclusions: Customized task-oriented training can be implemented to accelerate gains across a full spectrum of patient-reported outcomes. While group differences for most outcomes disappeared at 1 year, ASAP participants achieved these outcomes on average 8 months earlier (ClinicalTrials.gov: Interdisciplinary Comprehensive Arm Rehabilitation Evaluation [ICARE] Stroke Initiative, at www.ClinicalTrials.gov/ClinicalTrials.gov . Identifier: NCT00871715).
Keywords: International Classification of Disability and Functioning (ICF); patient-centered; quality of life; rehabilitation; task-oriented.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Mayo NE, Wood-Dauphinee S, Cote´ R, Durcan L, Carlton J. Activity, participation, and quality of life 6 months poststroke. Arch Phys Med Rehabil. 2002;83:1035–42. - PubMed
-
- Wolf SL, Lecraw DE, Barton LA, Jann BB. Forced use of hemiplegic upper extremities to reverse the effect of learned nonuse among chronic stroke and head injured patients. Exp Neurol. 1989;104:125–132. - PubMed
-
- Winstein CJ, Stein J, Arena R, et al. on behalf of the American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Quality of Care and Outcomes Research. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47:e98–e169. doi: 10.1161/STR.0000000000000098. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
