

Pretreatment prognostic factors of survival and late toxicities for patients with nasopharyngeal carcinoma treated by simultaneous integrated boost intensity-modulated radiotherapy
- PMID: 29554940
- PMCID: PMC5859644
- DOI: 10.1186/s13014-018-0990-5
Pretreatment prognostic factors of survival and late toxicities for patients with nasopharyngeal carcinoma treated by simultaneous integrated boost intensity-modulated radiotherapy
Abstract
Background: To scrutinize the pretreatment prognosticators on survival and late toxicities in a homogenous cohort of nasopharyngeal carcinoma (NPC) patients treated by simultaneous integrated boost intensity-modulated radiation therapy (SIB-IMRT).
Methods: A total of 219 non-distant metastatic NPC patients consecutively treated by SIB-IMRT at a single institute were collected. The pretreatment factors including the socio-demographic variables, TNM stages, gross tumor volume (GTV), Epstein-Barr virus (EBV)-DNA, and hematologic inflammatory markers were analyzed. Cox model was used to screen the prognostic factors of late toxicities and four survival outcomes including locoregional relapse-free survival (LRRFS), distant metastasis-free survival (DMFS), failure-free survival (FFS), and overall survival (OS).
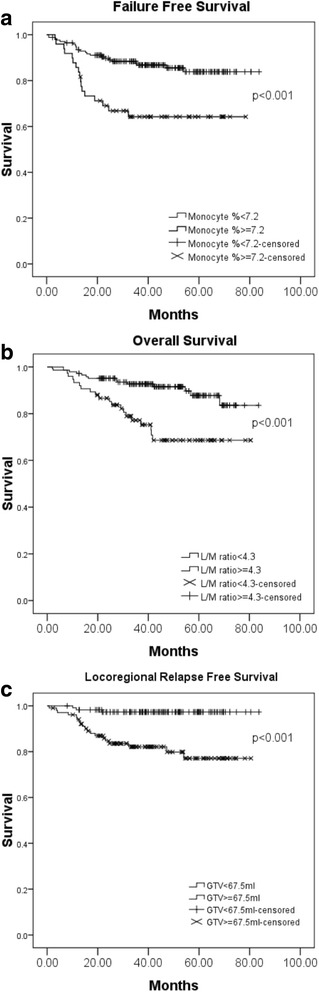
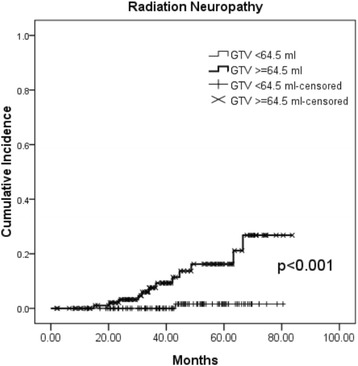
Results: Statistically significant inter-correlations were observed between the values of EBV-DNA, some hematologic inflammatory markers, GTV, and N classification. The 5-year LRRFS, DMFS, FFS, and OS rates were 87.9%, 89.4%, 79.4%, and 81.3%, respectively. Multivariate analysis revealed that advanced N classification (N2-3 vs. N0-1) remained the only significant negative prognosticator for all the four survival outcomes. An increased monocyte percentage and a decreased lymphocyte-to-monocyte ratio were significantly associated with poorer FFS and OS, respectively. Larger GTV was observed to be predictive of poorer LRRFS. Patients with T3-4 (HR: 3.5, 95% CI: 1.0-12.1, p = 0.048) or higher GTV (HR: 1.006, 95% CI: 1.001-1.011, p = 0.027) were associated with higher incidence of radiation neuropathy.
Conclusion: N classification remains the most significant survival predictor for NPC patients treated by SIB-IMRT after adjusting these biomarkers. GTV impacts not only on locoregional control but also radiation neuropathy.
Keywords: Epstein-Barr virus DNA; Gross tumor volume; Hematologic inflammatory marker; Nasopharyngeal carcinoma; Simultaneous integrated boost intensity-modulated radiation therapy.
Conflict of interest statement
Ethics approval and consent to participate
This study obtained ethics approval from the Institutional review board/Ethics committee (IRB/EC) of Kaohsiung Chang Gung Memorial Hospital.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Treatment outcomes and late toxicities of 869 patients with nasopharyngeal carcinoma treated with definitive intensity modulated radiation therapy: new insight into the value of total dose of cisplatin and radiation boost.Oncotarget. 2015 Nov 10;6(35):38381-97. doi: 10.18632/oncotarget.5420. Oncotarget. 2015. PMID: 26485757 Free PMC article.
-
Prognostic value of gross tumor regression and plasma Epstein Barr Virus DNA levels at the end of intensity-modulated radiation therapy in patients with nasopharyngeal carcinoma.Radiother Oncol. 2019 Mar;132:223-229. doi: 10.1016/j.radonc.2018.10.010. Epub 2018 Oct 23. Radiother Oncol. 2019. PMID: 30366725
-
Survival analysis of patients with advanced-stage nasopharyngeal carcinoma according to the Epstein-Barr virus status.Oncotarget. 2016 Apr 26;7(17):24208-16. doi: 10.18632/oncotarget.8144. Oncotarget. 2016. PMID: 27008701 Free PMC article.
-
The effectiveness of intensity-modulated radiation therapy versus 2D-RT for the treatment of nasopharyngeal carcinoma: A systematic review and meta-analysis.PLoS One. 2019 Jul 10;14(7):e0219611. doi: 10.1371/journal.pone.0219611. eCollection 2019. PLoS One. 2019. PMID: 31291379 Free PMC article.
-
Long-term outcomes after reirradiation in nasopharyngeal carcinoma with intensity-modulated radiotherapy: A meta-analysis.Head Neck. 2018 Mar;40(3):622-631. doi: 10.1002/hed.24993. Epub 2017 Nov 11. Head Neck. 2018. PMID: 29130584 Review.
Cited by
-
Comparison of radiomics tools for image analyses and clinical prediction in nasopharyngeal carcinoma.Br J Radiol. 2019 Oct;92(1102):20190271. doi: 10.1259/bjr.20190271. Epub 2019 Aug 27. Br J Radiol. 2019. PMID: 31453720 Free PMC article.
-
Correlation of serum IL-2 and IFN-γ levels with clinical prognosis of nasopharyngeal carcinoma patients and analysis of risk factors.J Med Biochem. 2024 Jan 25;43(1):50-56. doi: 10.5937/jomb0-44057. J Med Biochem. 2024. PMID: 38496017 Free PMC article.
-
Toripalimab plus intensity-modulated radiotherapy for recurrent nasopharyngeal carcinoma: an open-label single-arm, phase II trial.J Immunother Cancer. 2021 Nov;9(11):e003290. doi: 10.1136/jitc-2021-003290. J Immunother Cancer. 2021. PMID: 34782428 Free PMC article. Clinical Trial.
-
Negative Prognostic Impact of Smoking on Long-term Survival in Patients With Nasopharyngeal Carcinoma Treated With Curative (Chemo)radiotherapy.In Vivo. 2023 Jul-Aug;37(4):1775-1785. doi: 10.21873/invivo.13266. In Vivo. 2023. PMID: 37369456 Free PMC article.
-
Comparing the 7th and 8th editions of UICC/AJCC staging system for nasopharyngeal carcinoma in the IMRT era.BMC Cancer. 2021 Mar 30;21(1):327. doi: 10.1186/s12885-021-08036-8. BMC Cancer. 2021. PMID: 33785010 Free PMC article.
References
-
- Songthong AP, Kannarunimit D, Chakkabat C, Lertbutsayanukul C. A randomized phase II/III study of adverse events between sequential (SEQ) versus simultaneous integrated boost (SIB) intensity modulated radiation therapy (IMRT) in nasopharyngeal carcinoma; preliminary result on acute adverse events. Radiat Oncol. 2015;10:166. doi: 10.1186/s13014-015-0472-y. - DOI - PMC - PubMed
-
- Lee N, Harris J, Garden AS, Straube W, Glisson B, Xia P, et al. Intensity-modulated radiation therapy with or without chemotherapy for nasopharyngeal carcinoma: radiation therapy oncology group phase II trial 0225. J Clin Oncol. 2009;27(22):3684–3690. doi: 10.1200/JCO.2008.19.9109. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
