

Basic vs More Complex Definitions of Family History in the Prediction of Coronary Heart Disease: The Multi-Ethnic Study of Atherosclerosis
- PMID: 29555305
- PMCID: PMC6129200
- DOI: 10.1016/j.mayocp.2018.01.014
Basic vs More Complex Definitions of Family History in the Prediction of Coronary Heart Disease: The Multi-Ethnic Study of Atherosclerosis
Abstract
Objective: To determine whether family history of coronary heart disease (FH) definitions differ in their association with atherosclerotic cardiovascular disease (ASCVD) events.
Patients and methods: Participants who provided FH data from July 17, 2000, through February 24, 2004, were identified. Definitions of FH were any, premature, and Familial Risk Assessment (FRA). Outcomes included coronary heart disease (CHD), stroke, peripheral artery disease, angina, and congestive heart failure. Multivariable-adjusted Cox models examined the association of FH definitions with events. C statistics and the net reclassification index examined the incremental prognostic contribution of each definition.
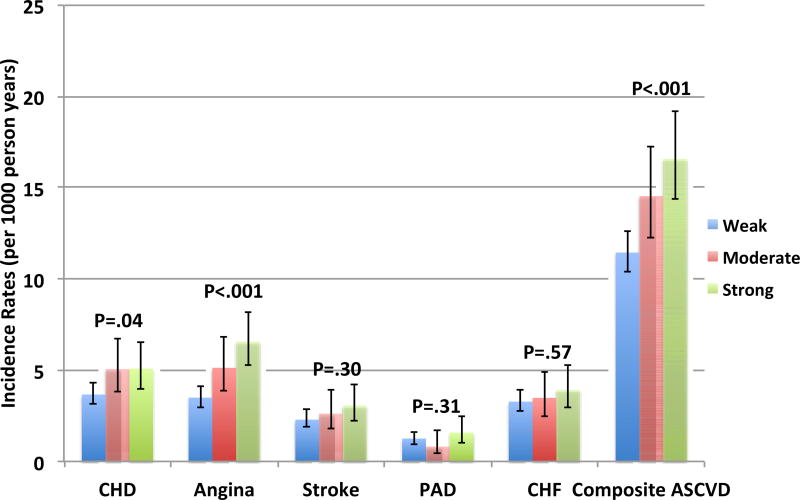
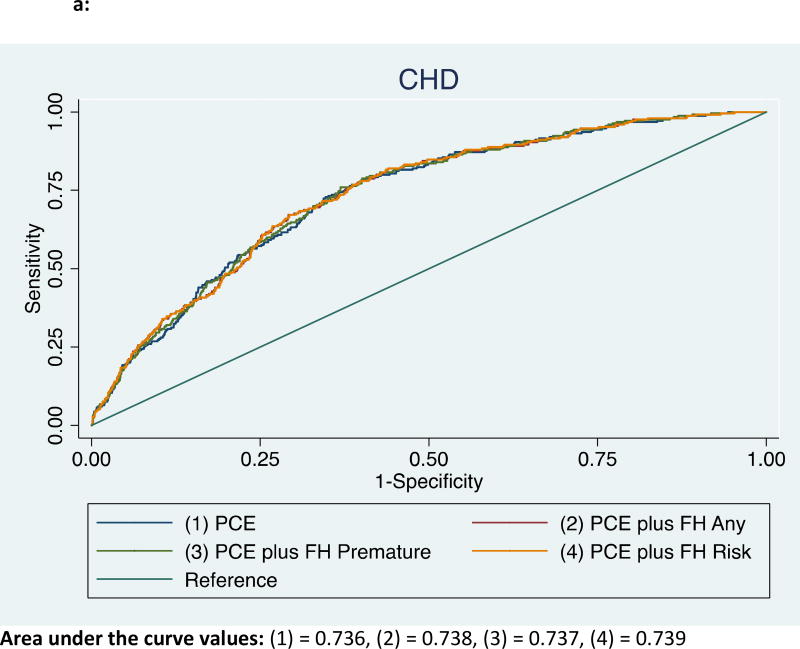
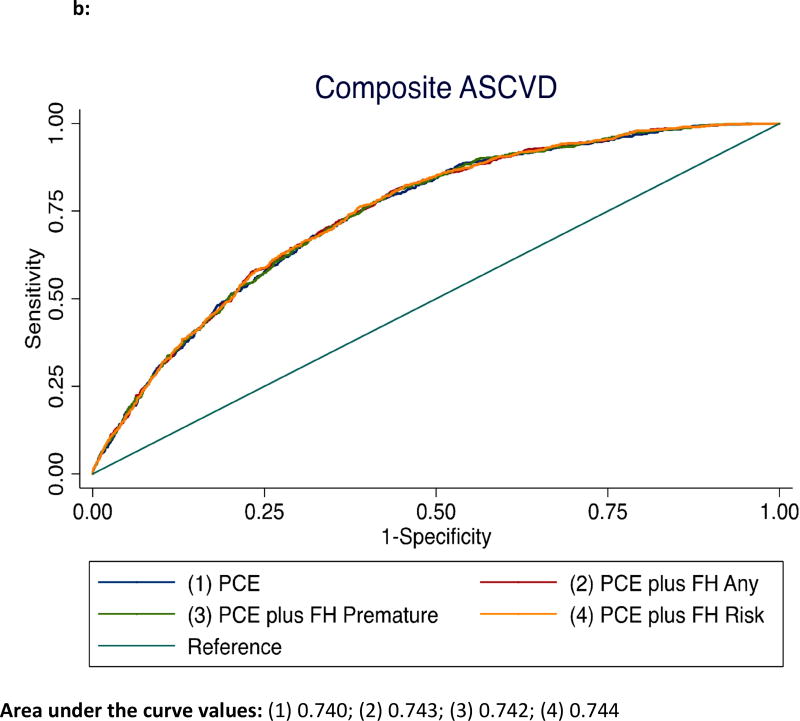
Results: In 6200 participants, the proportions of any FH and premature FH were 36% and 16%, respectively, and of weak, moderate, and strong familial risk were 20%, 16%, and 20%, respectively. Over median follow-up of 10.1 years (range, 0.02-11.5 years), 741 participants experienced a composite event. Compared with no FH, any FH was associated with incident CHD, angina, and composite ASCVD (hazard ratios [95% CIs]: 1.4 [1.1-1.8], 1.6 [1.2-2.1], and 1.3 [1.1-1.5], respectively). Similar results were obtained for premature FH compared with no FH and for strong compared with weak FRA for these 3 outcomes. There was no association between the FH definitions and noncoronary cardiovascular events. Compared with traditional risk factors (C statistic = 0.740), any FH, premature FH, and FRA all improved discrimination of composite ASCVD (all P < .01); however, the differences in C statistics among any FH (0.743), premature FH (0.742), and FRA (0.744) were numerically small, as were differences in the net reclassification index.
Conclusion: A single question regarding the presence of FH in any first-degree relative performs just as well as more complicated assessments in predicting CHD.
Trial registration: clinicaltrials.gov Identifier: NCT00005487.
Copyright © 2018 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Drs. Patel, Al Rifai, Shea, Blumenthal, Blaha, and McEvoy do not have any disclosures to report.
Figures
Comment in
-
Family History of Cardiovascular Disease: How Detailed Should It Be?Mayo Clin Proc. 2018 Sep;93(9):1167-1168. doi: 10.1016/j.mayocp.2018.07.010. Epub 2018 Aug 7. Mayo Clin Proc. 2018. PMID: 30093169 No abstract available.
References
-
- Safarova MS, Bailey KR, Kullo IJ. Association of a Family History of Coronary Heart Disease with Initiation of Statin Therapy in Individuals at Intermediate Risk: Post Hoc Analysis of a Randomized Clinical Trial. JAMA Cardiol. 2016;1(3):364–366. - PubMed
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 Pt B):2935–2959. - PMC - PubMed
-
- Sesso HD, Lee IM, Gaziano JM, et al. Maternal and paternal history of myocardial infarction and risk of cardiovascular disease in men and women. Circulation. 2001;104(4):393–398. - PubMed
-
- Lloyd-Jones DM, Nam BH, D'Agostino RB, Sr, et al. Parental cardiovascular disease as a risk factor for cardiovascular disease in middle-aged adults: a prospective study of parents and offspring. JAMA. 2004;291(18):2204–2211. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- N01HC95169/HL/NHLBI NIH HHS/United States
- N01HC95161/HL/NHLBI NIH HHS/United States
- N01HC95162/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01HC95165/HL/NHLBI NIH HHS/United States
- N01HC95167/HL/NHLBI NIH HHS/United States
- N01HC95163/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- N01HC95160/HL/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- N01HC95164/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01HC95166/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
