

Anatomical and procedural determinants of ambulatory blood pressure lowering following catheter-based renal denervation using radiofrequency
- PMID: 29555535
- PMCID: PMC6667167
- DOI: 10.1016/j.carrev.2018.02.016
Anatomical and procedural determinants of ambulatory blood pressure lowering following catheter-based renal denervation using radiofrequency
Abstract
Background/purpose: Catheter-based renal sympathetic denervation (RDN) has been introduced to lower blood pressure (BP) and sympathetic activity in patients with uncontrolled hypertension with at best equivocal results. It has been postulated that anatomic and procedural elements introduce unaccounted variability and yet little is known of the impact of renal anatomy and procedural parameters on BP response to RDN.
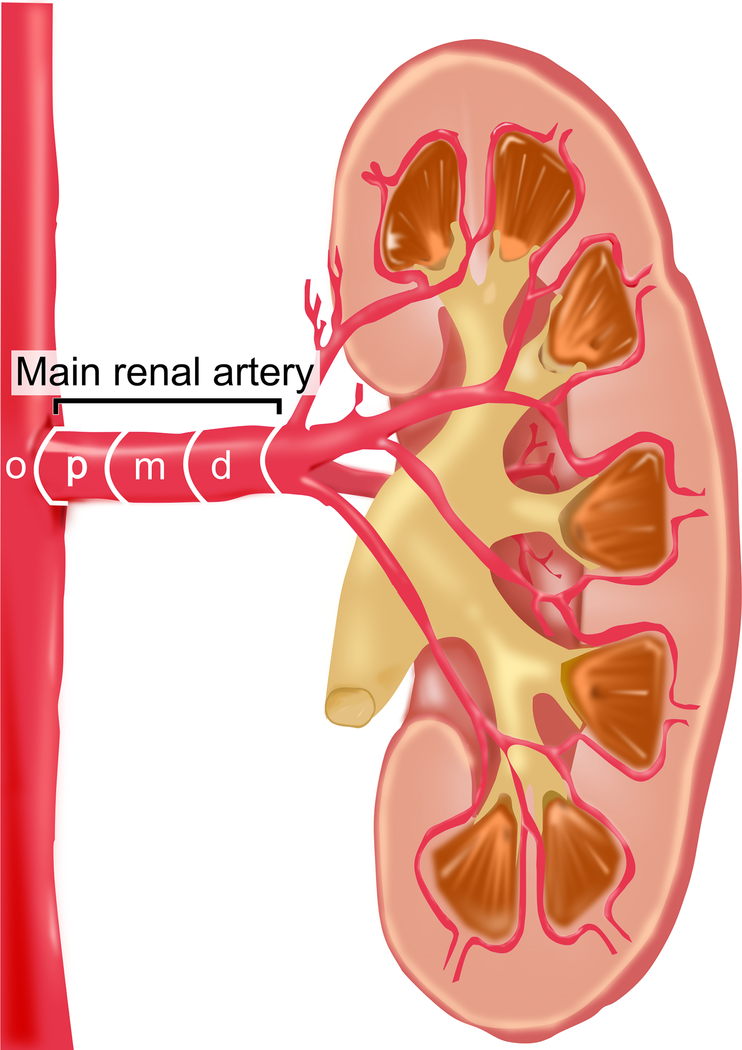
Methods/materials: Anatomical parameters such as length and diameter were analyzed by quantitative vascular analysis and the prevalence of accessory renal arteries and renal artery disease were documented in 150 patients with resistant hypertension undergoing bilateral RDN using a mono-electrode radiofrequency catheter (Symplicity Flex, Medtronic).
Results: Accessory renal arteries and renal artery disease were present in 56 (37%) and 14 patients (9%), respectively. At 6-months, 24 h-ambulatory BP was reduced by 11/6 mm Hg (p < 0.001 for both). Change of systolic blood pressure (SBP) was not related to the presence of accessory renal arteries (p = 0.543) or renal artery disease (p = 0.598). Patients with at least one main renal artery diameter ≤ 4 mm had a more pronounced reduction of 24 h-ambulatory SBP compared to patients where both arteries were >4 mm (-19 vs. -10 mmHg; p = 0.038). Neither the length of the renal artery nor the number of RF ablations influenced 24 h-ambulatory BP reduction at 6 months.
Conclusions: 24 h-ambulatory BP lowering was most pronounced in patients with smaller renal artery diameter but not related to renal artery length, accessory arteries or renal artery disease. Further, there was no dose-response relationship observed with increasing number of ablations.
Condensed abstract: Because little is known of the impact of renal anatomy and procedural parameters on blood pressure (BP) response to renal denervation (RDN), anatomical and procedural data were analyzed in 150 patients undergoing bilateral RDN. BP lowering was most pronounced in patients with smaller renal artery diameter but not related to renal artery length, the presence of renal artery disease or accessory renal arteries. Further, there was no dose-response relationship observed with increasing number of ablations.
Keywords: Ambulatory blood pressure; Anatomical; Procedural determinants; Renal denervation.
Copyright © 2018. Published by Elsevier Inc.
Figures



References
-
- Mahfoud F, Bohm M, Azizi M, Pathak A, Durand Zaleski I, Ewen S, et al. Proceedings from the European clinical consensus conference for renal denervation: considerations on future clinical trial design. Eur Heart J 2015; 36:2219–2227. - PubMed
-
- Krum H, Schlaich MP, Whitbourn R, Sobotka PA, Sadowski J, Bartus K, et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet 2009; 373:1275–1281. - PubMed
-
- Azizi M, Sapoval M, Gosse P, Monge M, Bobrie G, Delsart P, et al. Optimum and stepped care standardised antihypertensive treatment with or without renal denervation for resistant hypertension (DENERHTN): a multicentre, open-label, randomised controlled trial. Lancet 2015; 385:1957–1965. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
