

PIRCHE-II Is Related to Graft Failure after Kidney Transplantation
- PMID: 29556227
- PMCID: PMC5844930
- DOI: 10.3389/fimmu.2018.00321
PIRCHE-II Is Related to Graft Failure after Kidney Transplantation
Abstract
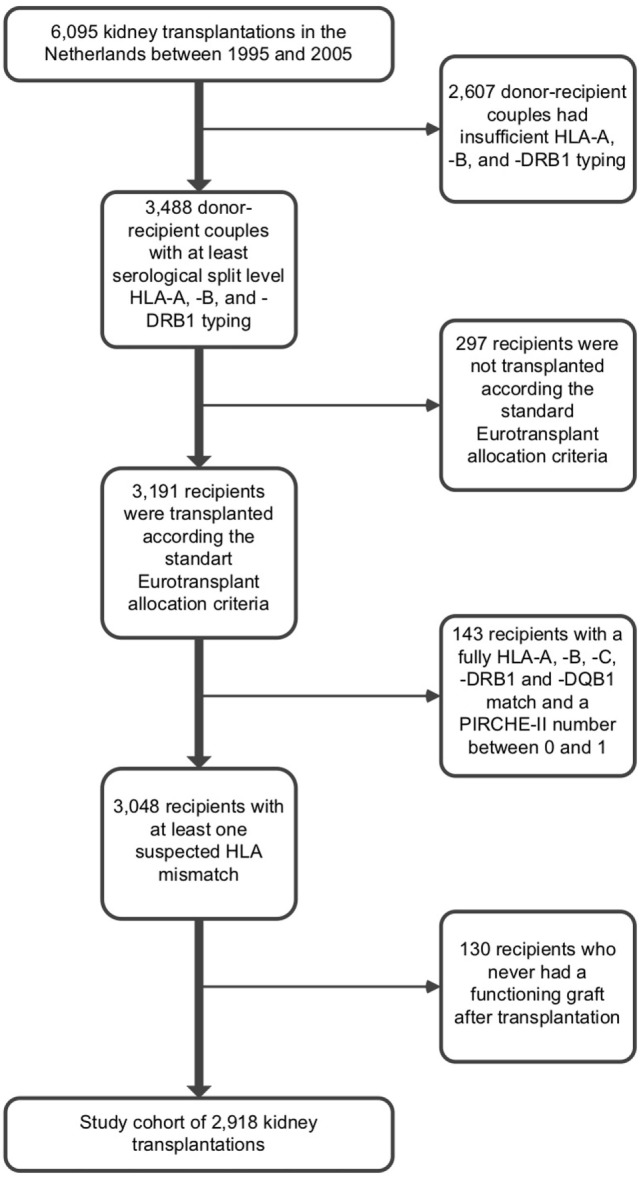
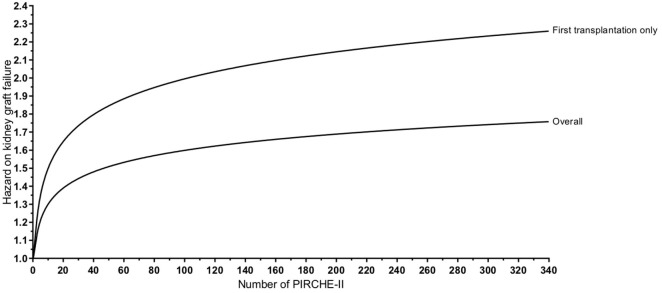
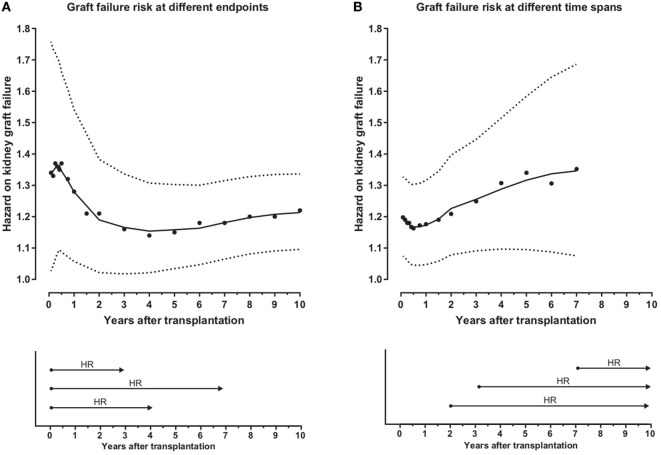
Individual HLA mismatches may differentially impact graft survival after kidney transplantation. Therefore, there is a need for a reliable tool to define permissible HLA mismatches in kidney transplantation. We previously demonstrated that donor-derived Predicted Indirectly ReCognizable HLA Epitopes presented by recipient HLA class II (PIRCHE-II) play a role in de novo donor-specific HLA antibodies formation after kidney transplantation. In the present Dutch multi-center study, we evaluated the possible association between PIRCHE-II and kidney graft failure in 2,918 donor-recipient couples that were transplanted between 1995 and 2005. For these donors-recipients couples, PIRCHE-II numbers were related to graft survival in univariate and multivariable analyses. Adjusted for confounders, the natural logarithm of PIRCHE-II was associated with a higher risk for graft failure [hazard ratio (HR): 1.13, 95% CI: 1.04-1.23, p = 0.003]. When analyzing a subgroup of patients who had their first transplantation, the HR of graft failure for ln(PIRCHE-II) was higher compared with the overall cohort (HR: 1.22, 95% CI: 1.10-1.34, p < 0.001). PIRCHE-II demonstrated both early and late effects on graft failure in this subgroup. These data suggest that the PIRCHE-II may impact graft survival after kidney transplantation. Inclusion of PIRCHE-II in donor-selection criteria may eventually lead to an improved kidney graft survival.
Keywords: HLA antigens; HLA matching; PIRCHE-II; graft rejection; kidney transplantation.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials