

Long-term analysis of 2 prospective studies that incorporate mitomycin C into an adjuvant chemoradiation regimen for pancreatic and periampullary cancers
- PMID: 29556579
- PMCID: PMC5856978
- DOI: 10.1016/j.adro.2017.07.008
Long-term analysis of 2 prospective studies that incorporate mitomycin C into an adjuvant chemoradiation regimen for pancreatic and periampullary cancers
Abstract
Purpose: The purpose of this study was to report toxicity and long-term survival outcomes of 2 prospective trials evaluating mitomycin C (MMC) with 5-fluorouracil-based adjuvant chemoradiation in resected periampullary adenocarcinoma.
Methods and materials: From 1996 to 2002, 119 patients received an adjuvant 4-drug chemotherapy regimen of 5-fluorouracil, leucovorin, MMC, and dipyridamole with chemoradiation on 2 consecutive trials (trials A and B). Trial A patients received upfront chemoradiation (50 Gy split-course, 2.5 Gy/fraction) followed by 4 cycles of the 4-drug chemotherapy with bolus 5-fluorouracil. Trial B patients received 1 cycle of the 4-drug chemotherapy with continuous infusion 5-fluorouracil followed by continuous chemoradiation (45-54 Gy, 1.8 Gy/fraction) and 2 additional cycles of chemotherapy. Cox proportional hazards models were performed to identify prognostic factors for overall survival (OS).
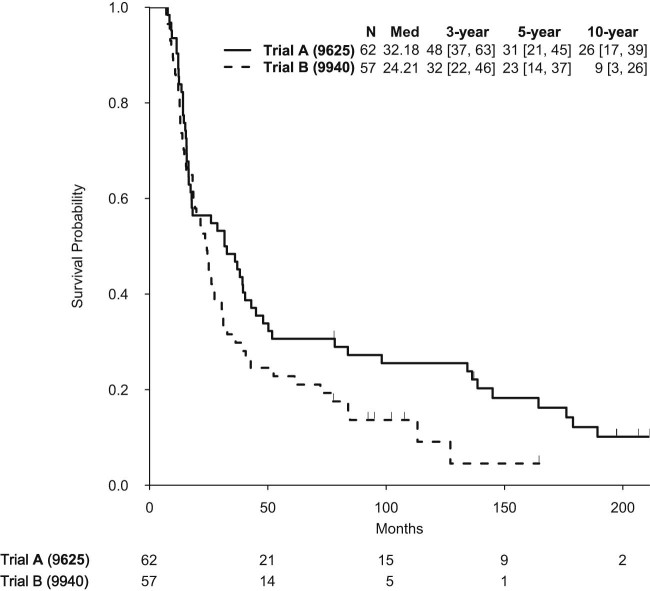
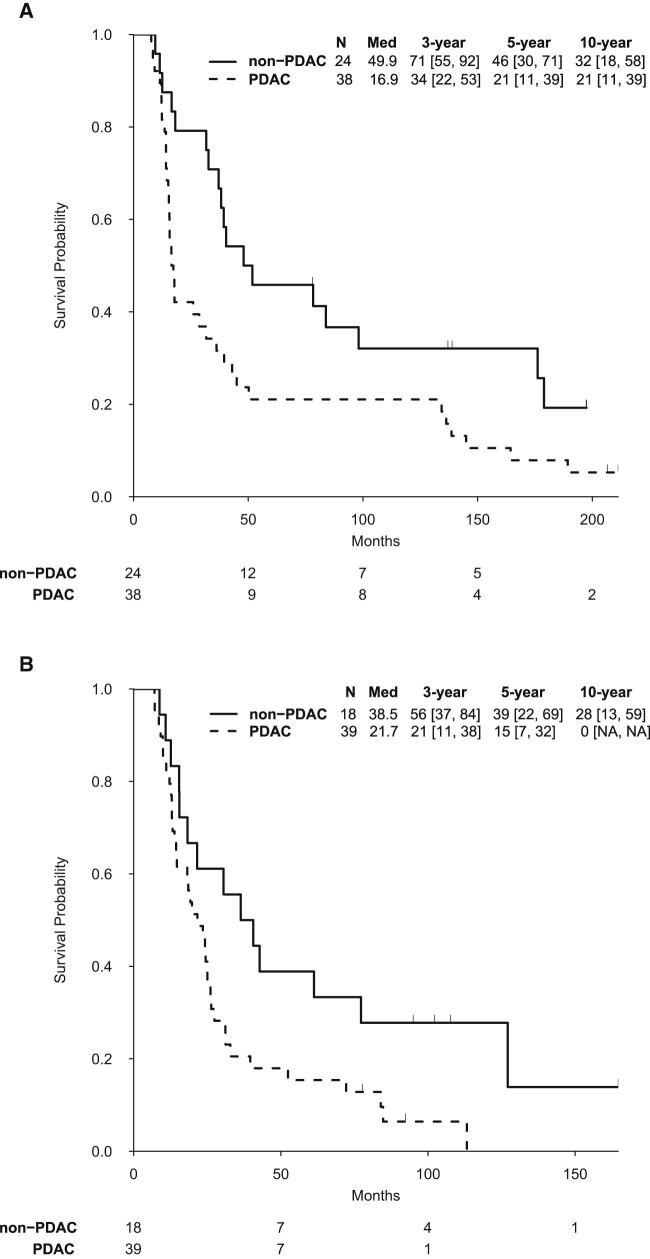
Results: Of the 62 trial A patients, 61% had pancreatic and 39% nonpancreatic periampullary carcinomas. Trial B (n = 57) consisted of 68% pancreatic and 32% nonpancreatic periampullary carcinomas. Resection margin and lymph node status were similar for both trials. Median follow-up was longer for trial A than trial B (197.5 vs 107.0 months), with median OS of 32.2 and 24.2 months, respectively. Rates of 3-, 5-, and 10-year OS were 48%, 31%, and 26% in trial A and 32%, 23%, and 9% in trial B. On multivariate analysis, lymph node-positive resection was the strongest prognostic factor for OS. A pancreatic primary and positive margin status were also associated with inferior survival (P < .05). Rates of grade ≥3 treatment-related toxicity in trials A and B were 2% and 7%, respectively.
Conclusions: This is the first study to report long-term outcomes of MMC with 5-fluorouracil-based adjuvant chemoradiation in periampullary cancers. Because MMC may be considered in DNA repair-deficient carcinomas, randomized trials are needed to determine the true benefit of adjuvant MMC.
Figures
References
-
- Chakravarthy A., Abrams R.A., Yeo C.J. Intensified adjuvant combined modality therapy for resected periampullary adenocarcinoma: Acceptable toxicity and suggestion of improved 1-year disease-free survival. Int J Radiat Oncol Biol Phys. 2000;48:1089–1096. - PubMed
-
- Morak M.J., van der Gaast A., Incrocci L. Adjuvant intra-arterial chemotherapy and radiotherapy versus surgery alone in resectable pancreatic and periampullary cancer: A prospective randomized controlled trial. Ann Surg. 2008;248:1031–1041. - PubMed
-
- Gutierrez J.C., Franceschi D., Koniaris L.G. How many lymph nodes properly stage a periampullary malignancy? J Gastrointest Surg. 2008;12:77–85. - PubMed
-
- Neoptolemos J.P., Moore M.J., Cox T.F. Effect of adjuvant chemotherapy with fluorouracil plus folinic acid or gemcitabine vs observation on survival in patients with resected periampullary adenocarcinoma: The ESPAC-3 periampullary cancer randomized trial. JAMA. 2012;308:147–156. - PubMed
-
- Aiura K., Takahashi S., Matsui J., Ueda M., Kitagawa Y. Beneficial effects of 5-fluorouracil and heparin-based portal infusion chemotherapy combined with mitomycin C and cisplatin after curative resection of pancreatic cancer. Pancreatology. 2010;10:250–258. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
