

Value of electronic alerts for acute kidney injury in high-risk wards: a pilot randomized controlled trial
- PMID: 29556903
- PMCID: PMC6096658
- DOI: 10.1007/s11255-018-1836-7
Value of electronic alerts for acute kidney injury in high-risk wards: a pilot randomized controlled trial
Abstract
Purpose: To investigate the application value of "electronic alerts" ("e-alerts") for acute kidney injury (AKI) among high-risk wards of hospitals.
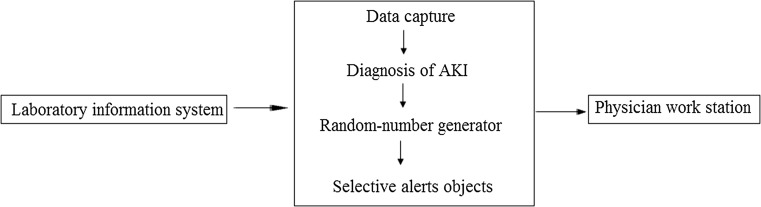
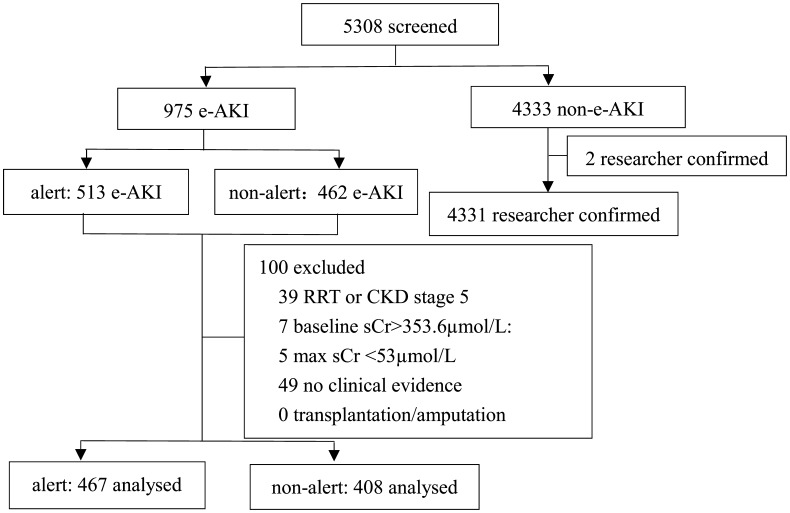
Methods: A prospective, randomized, controlled study was conducted. We developed an e-alert system for AKI and ran the system in intensive care units and divisions focusing on cardiovascular disease. The e-alert system diagnosed AKI automatically based on serum creatinine levels. Patients were assigned randomly to an e-alert group (467 patients) or non-e-alert group (408 patients). Only the e-alert group could receive pop-up messages.
Results: The sensitivity, specificity, Youden Index and accuracy of the AKI e-alert system were 99.8, 97.7, 97.5 and 98.1%, respectively. The prevalence of the diagnosis for AKI and expanded-AKI (AKI or multiple-organ failure) in the e-alert group was higher than that in the non-e-alert group (AKI 7.9 and 2.7%, P = 0.001; expanded-AKI 16.3 and 6.1%, P < 0.001). The prevalence of nephrology consultation in the e-alert group was higher than that in the non-e-alert group (9.0 and 3.7%, P = 0.001). There was no significant difference in the prevalence dialysis, rehabilitation of renal function or death in the two groups.
Conclusion: The e-alert system described here was a reliable tool to make an accurate diagnosis of AKI.
Keywords: Acute kidney injury; Diagnosis; Information system; Surveillance; e-alert.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
