

Proceedings of the NASHNP Companion Meeting, March 18th, 2018, Vancouver, BC, Canada: Salivary Neuroendocrine Carcinoma-An Overview of a Rare Disease with an Emphasis on Determining Tumor Origin
- PMID: 29556963
- PMCID: PMC5873497
- DOI: 10.1007/s12105-018-0896-4
Proceedings of the NASHNP Companion Meeting, March 18th, 2018, Vancouver, BC, Canada: Salivary Neuroendocrine Carcinoma-An Overview of a Rare Disease with an Emphasis on Determining Tumor Origin
Abstract
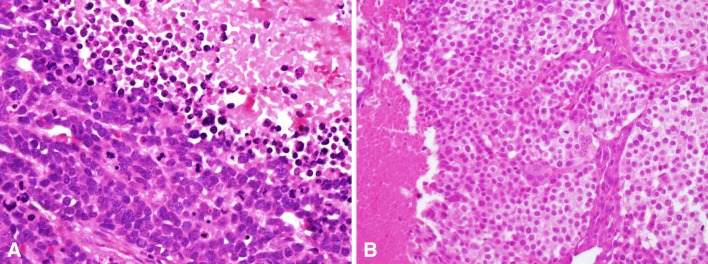
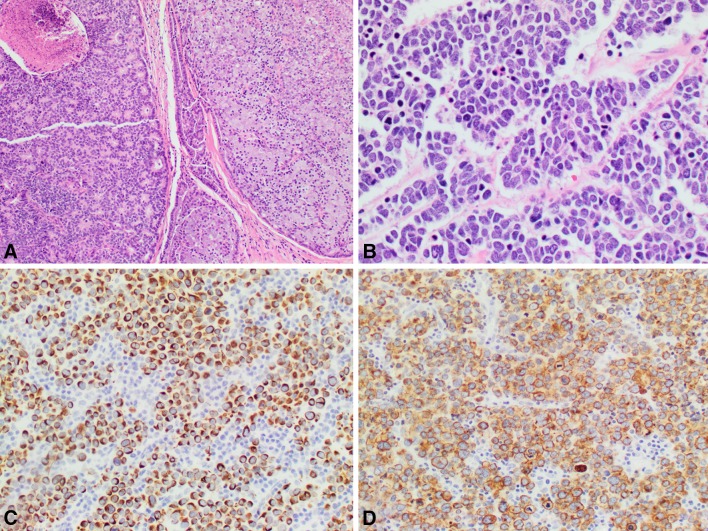
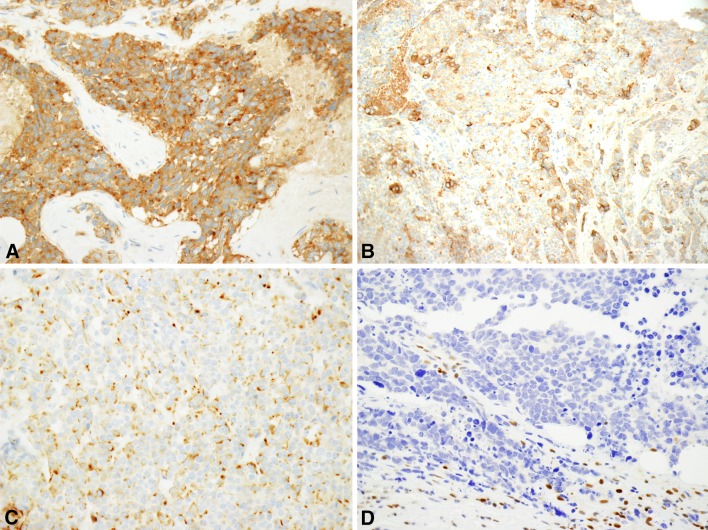
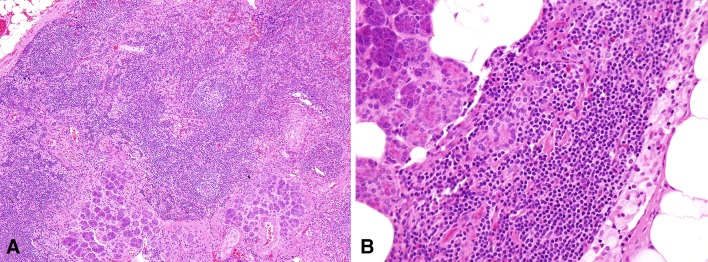
Salivary neuroendocrine carcinomas are rare and the overwhelming majority is high-grade. The parotid gland is the most commonly involved site followed by the submandibular gland. Most arise de novo but rare examples occurring as a high-grade transformation of another type of salivary gland neoplasm exist. There is significant morphologic and immunophenotypic overlap with neuroendocrine carcinomas of other sites, especially the skin. Like cutaneous neuroendocrine (or Merkel cell) carcinomas, approximately three-fourths are cytokeratin 20 positive. Cytokeratin 20 positive salivary neuroendocrine carcinomas are often referred to as being of the 'Merkel cell type' since most other non-cutaneous neuroendocrine carcinomas are cytokeratin 20 negative. Salivary neuroendocrine carcinomas may be challenging to separate from Merkel cell carcinomas of the head and neck on pathologic grounds because the latter often metastasize to the parotid gland. Clinical history is often relied upon to separate primary salivary tumors from cutaneous metastases but may not be helpful in all cases. Here we review the clinical, pathologic and molecular features of salivary neuroendocrine carcinomas focusing on high-grade major salivary gland tumors. The difficulty in separating salivary tumors from metastatic Merkel cell carcinoma will be highlighted.
Keywords: Large cell neuroendocrine carcinoma; Merkel cell carcinoma; Merkel cell polyomavirus; Neuroendocrine carcinoma; Salivary; Small cell carcinoma.
Conflict of interest statement
The authors have no sources of funding or conflicts of interest to disclose.
Figures
References
-
- Mair S, Phillips JI, Cohen R. Small cell undifferentiated carcinoma of the parotid gland. Cytologic, histologic, immunohistochemical and ultrastructural features of a neuroendocrine variant. Acta Cytol. 1989;33:164–168. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
