

Cost and Cost-Effectiveness of a Demand Creation Intervention to Increase Uptake of Voluntary Medical Male Circumcision in Tanzania: Spending More to Spend Less
- PMID: 29557854
- PMCID: PMC6012046
- DOI: 10.1097/QAI.0000000000001682
Cost and Cost-Effectiveness of a Demand Creation Intervention to Increase Uptake of Voluntary Medical Male Circumcision in Tanzania: Spending More to Spend Less
Abstract
Background: Although voluntary medical male circumcision (VMMC) reduces the risk of HIV acquisition, demand for services is lower among men in most at-risk age groups (ages 20-34 years). A randomized controlled trial was conducted to assess the effectiveness of locally-tailored demand creation activities (including mass media, community mobilization, and targeted service delivery) in increasing uptake of campaign-delivered VMMC among men aged 20-34 years. We conducted an economic evaluation to understand the intervention's cost and cost-effectiveness.
Setting: Tanzania (Njombe and Tabora regions).
Methods: Cost data were collected on surgery, demand creation activities, and monitoring and supervision related to VMMC implementation across clusters in both trial arms, as well as start-up activities for the intervention arms. The Decision Makers' Program Planning Tool was used to estimate the number of HIV infections averted and related cost savings, given the total VMMCs per cluster. Disability-adjusted life years were calculated and used to estimate incremental cost-effectiveness ratios.
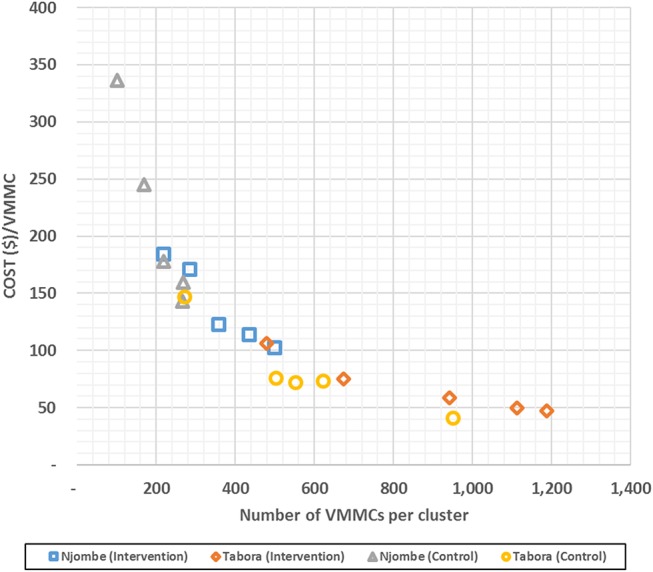
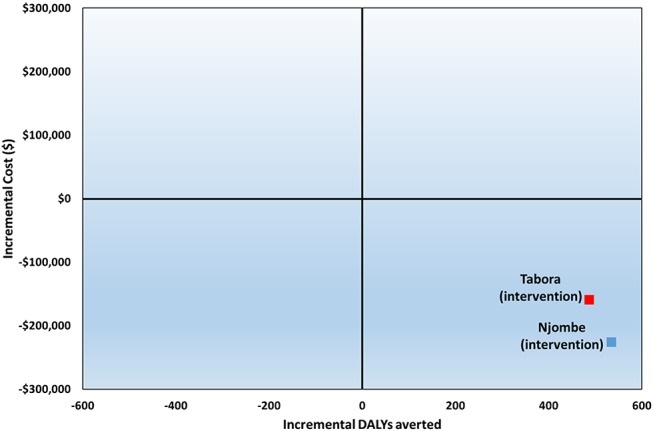
Results: Client load was higher in the intervention arms than in the control arms: 4394 vs. 2901 in Tabora and 1797 vs. 1025 in Njombe, respectively. Despite additional costs of tailored demand creation, demand increased more than proportionally: mean costs per VMMC in the intervention arms were $62 in Tabora and $130 in Njombe, and in the control arms $70 and $191, respectively. More infections were averted in the intervention arm than in the control arm in Tabora (123 vs. 67, respectively) and in Njombe (164 vs. 102, respectively). The intervention dominated the control because it was both less costly and more effective. Cost savings were observed in both regions stemming from the antiretroviral treatment costs averted as a result of the VMMCs performed.
Conclusions: Spending more to address local preferences as a way to increase uptake of VMMC can be cost-saving.
Figures
References
-
- Bailey RC, Moses S, Parker CB, et al. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet. 2007;369:643–656. - PubMed
-
- Gray RH, Kigozi G, Serwadda D, et al. Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. Lancet. 2007;369:657–666. - PubMed
-
- WHO, UNAIDS. New Data on Male Circumcision and HIV Prevention: Policy and Program Implications: Montreux, Switzerland: WHO, UNAIDS; 2007.
-
- World Health Organization. Voluntary Medical Male Circumcision for HIV Prevention in 14 Priority Countries in East and Southern Africa: Progress Brief June 2016.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
