

Solid Organ Transplantation in Patients With Preexisting Malignancies in Remission: A Propensity Score Matched Cohort Study
- PMID: 29557910
- PMCID: PMC7228636
- DOI: 10.1097/TP.0000000000002178
Solid Organ Transplantation in Patients With Preexisting Malignancies in Remission: A Propensity Score Matched Cohort Study
Abstract
Background: Solid-organ transplant recipients with pretransplant malignancies (PTM) have worse overall survival (OS) compared to recipients without history of malignancy. However, it is unknown whether the increased risk of mortality is due to recurrent cancer-related deaths.
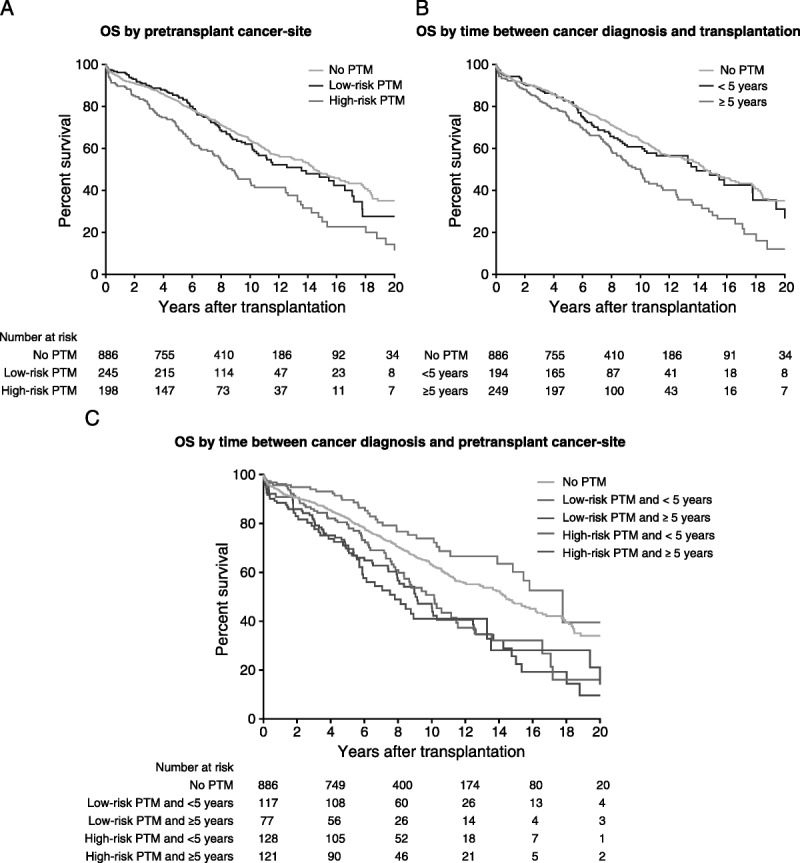
Methods: All solid-organ transplant recipients in Ontario between 1991 and 2010 were identified and matched 1:2 to recipients without PTM using a propensity score. OS was compared using the Kaplan-Meier estimator and Cox proportional hazard models. For cancer-specific mortality and cancer recurrence, cause-specific hazard models were used and the cumulative incidence was plotted.
Results: Recipients with PTM had a worse OS compared with recipients without PTM (median OS, 10.3 years vs 13.4 years). Recipients with PTM were not only at increased risk of cancer-specific mortality (cause-specific hazard ratio, 1.85; 95% confidence interval [CI], 1.20-2.86) but also at increased risk of noncancer death (cause-specific hazard ratio, 1.29; 95% CI, 1.08-1.54). Compared with recipients without PTM, recipients with high-risk PTM had higher all-cause mortality (hazard ratio, 1.81; 95% CI, 1.47-2.23). Recipients with low-risk PTM were not at increased risk (hazard ratio, 1.06; 95% CI, 0.86-1.31).
Conclusions: Recipients with PTM are at increased risk of all-cause mortality compared to recipients without PTM. This increased risk was noted for both cancer-specific and noncancer mortality. However, only those with high-risk PTM had worse outcomes.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures





Comment in
-
Preexisting Cancer in Transplant Candidates: Time for a Change in Practice?Transplantation. 2018 Jul;102(7):1037-1038. doi: 10.1097/TP.0000000000002177. Transplantation. 2018. PMID: 29557911 Free PMC article. No abstract available.
References
-
- Kasiske BL, Cangro CB, Hariharan S. The evaluation of renal transplantation candidates: clinical practice guidelines Am J Transplant 2001. 13–95 - PubMed
-
- Mehra MR, Kobashigawa J, Starling R. Listing criteria for heart transplantation: International Society for Heart and Lung Transplantation guidelines for the care of cardiac transplant candidates—2006 J Heart Lung Transplant 2006. 251024–1042 - PubMed
-
- Murray KF, Carithers RL. AASLD practice guidelines: evaluation of the patient for liver transplantation Hepatology 2005. 411407–1432 - PubMed
-
- Penn I. Evaluation of transplant candidates with pre-existing malignancies Ann Transplant 1997. 214–17 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
