

Metrics of early childhood growth in recent epidemiological research: A scoping review
- PMID: 29558499
- PMCID: PMC5860780
- DOI: 10.1371/journal.pone.0194565
Metrics of early childhood growth in recent epidemiological research: A scoping review
Abstract
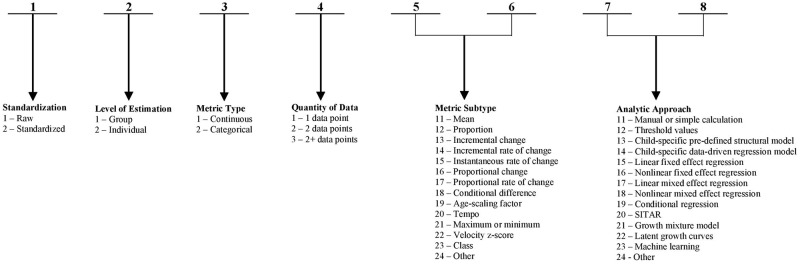
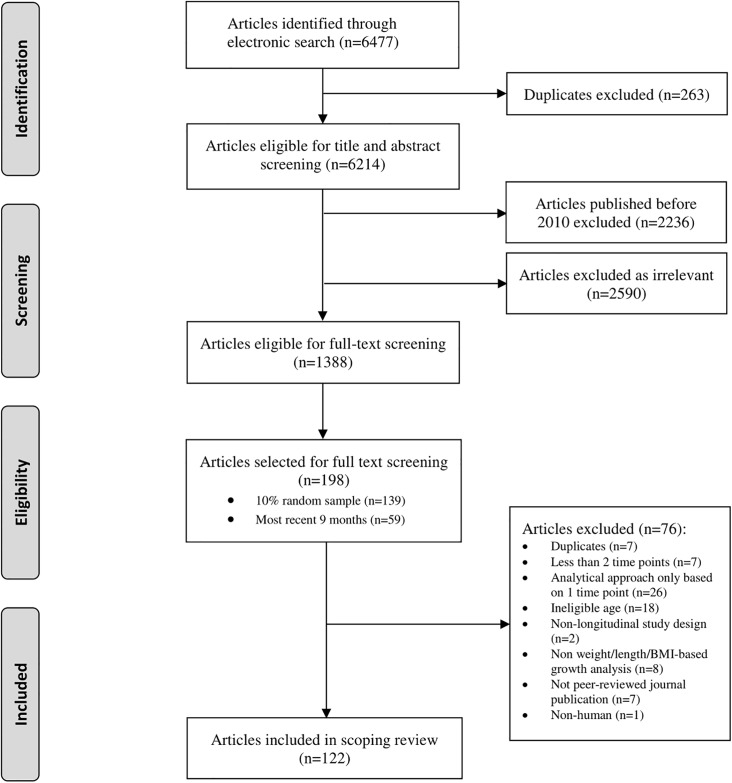
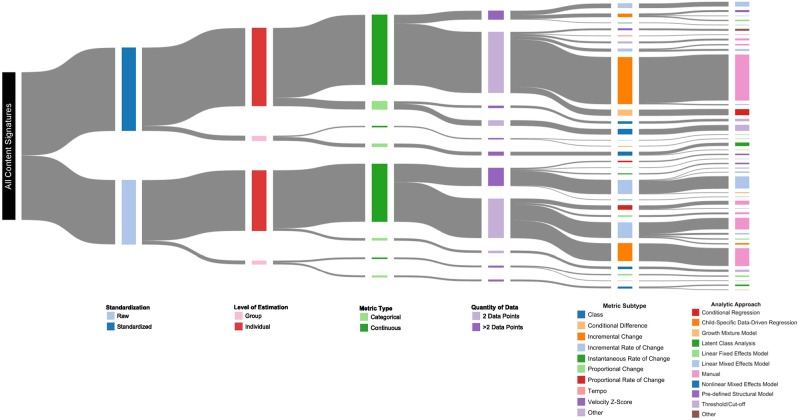
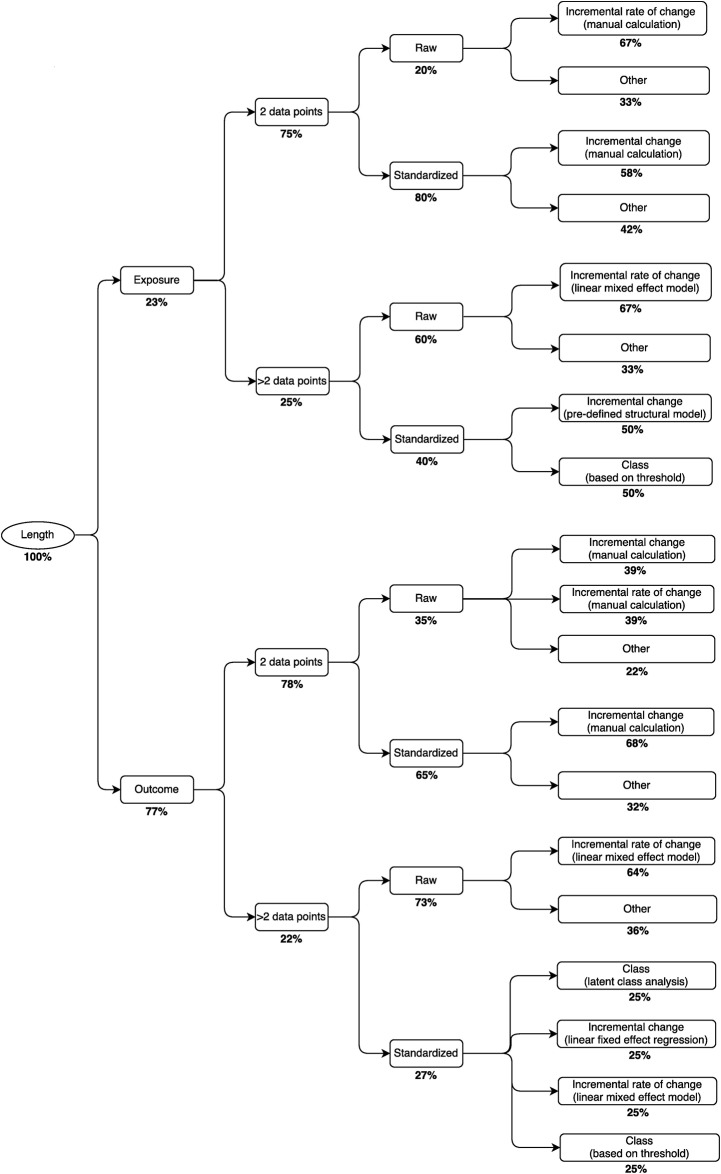
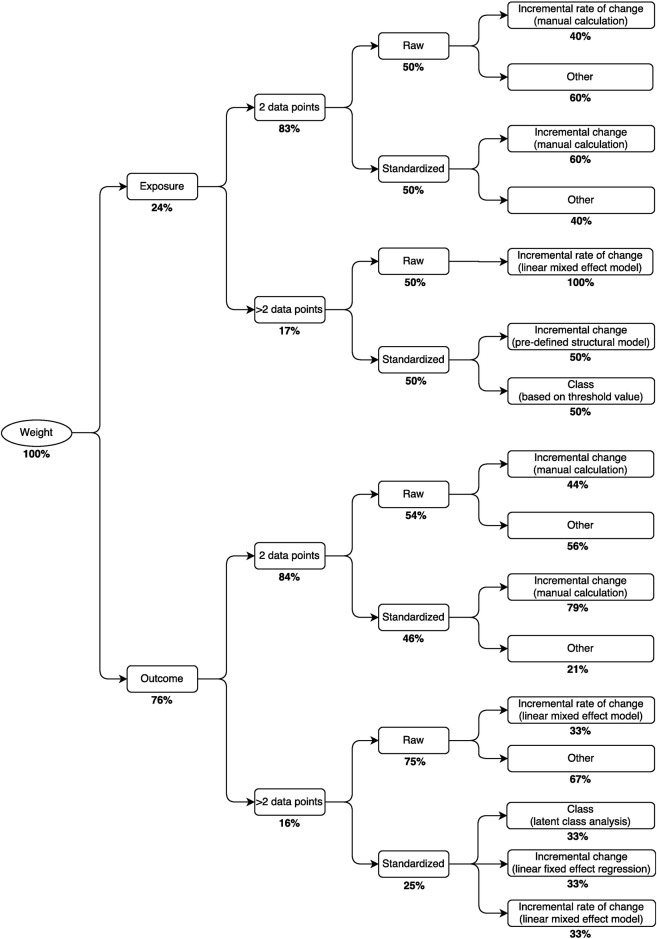
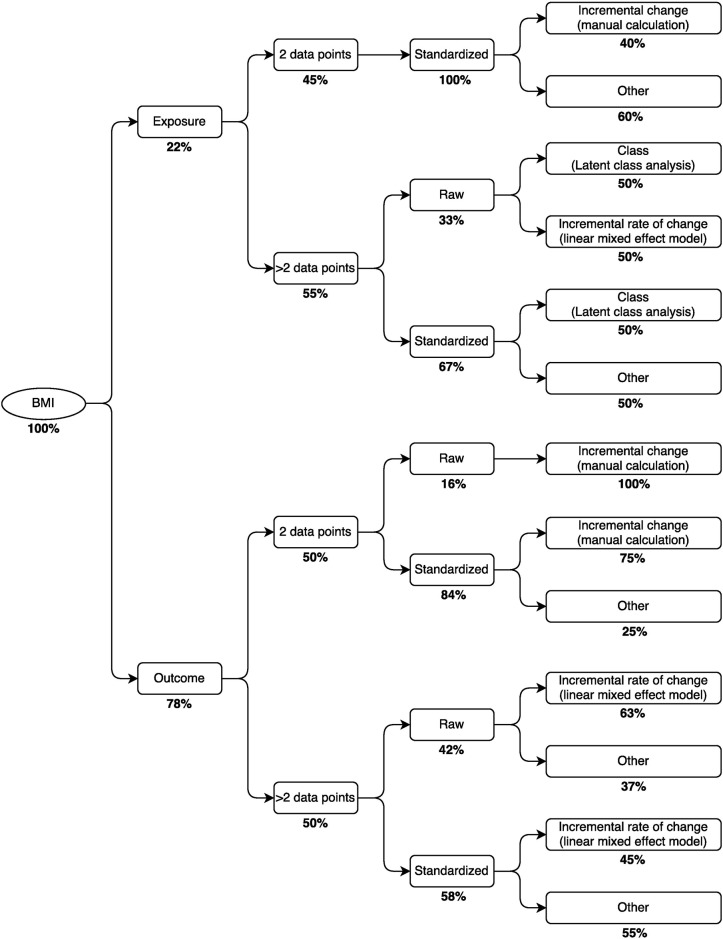
Metrics to quantify child growth vary across studies of the developmental origins of health and disease. We conducted a scoping review of child growth studies in which length/height, weight or body mass index (BMI) was measured at ≥ 2 time points. From a 10% random sample of eligible studies published between Jan 2010-Jun 2016, and all eligible studies from Oct 2015-June 2016, we classified growth metrics based on author-assigned labels (e.g., 'weight gain') and a 'content signature', a numeric code that summarized the metric's conceptual and statistical properties. Heterogeneity was assessed by the number of unique content signatures, and label-to-content concordance. In 122 studies, we found 40 unique metrics of childhood growth. The most common approach to quantifying growth in length, weight or BMI was the calculation of each child's change in z-score. Label-to-content discordance was common due to distinct content signatures carrying the same label, and because of instances in which the same content signature was assigned multiple different labels. In conclusion, the numerous distinct growth metrics and the lack of specificity in the application of metric labels challenge the integration of data and inferences from studies investigating the determinants or consequences of variations in childhood growth.
Conflict of interest statement
Figures
References
-
- Barker DJP. The developmental origins of adult disease. J Am Coll Nutr. 2004. December;23(6 Suppl):588S–595S. - PubMed
-
- Hui LL, Schooling CM, Leung SSL, Mak KH, Ho LM, Lam TH, et al. Birth weight, infant growth, and childhood body mass index: Hong Kong’s children of 1997 birth cohort. Arch Pediatr Adolesc Med. 2008. March;162(3):212–8. doi: 10.1001/archpediatrics.2007.62 - DOI - PubMed
-
- Baird J, Fisher D, Lucas P, Kleijnen J, Roberts H, Law C. Being big or growing fast: systematic review of size and growth in infancy and later obesity. BMJ. 2005;331(7522):929–0. doi: 10.1136/bmj.38586.411273.E0 - DOI - PMC - PubMed
-
- Stettler N, Zemel BS, Kumanyika S, Stallings VA. Infant weight gain and childhood overweight status in a multicenter, cohort study. Pediatrics. 2002. February;109(2):194–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
