

Impact of comorbidities on the prognoses of trauma patients: Analysis of a hospital-based trauma registry database
- PMID: 29558508
- PMCID: PMC5860791
- DOI: 10.1371/journal.pone.0194749
Impact of comorbidities on the prognoses of trauma patients: Analysis of a hospital-based trauma registry database
Abstract
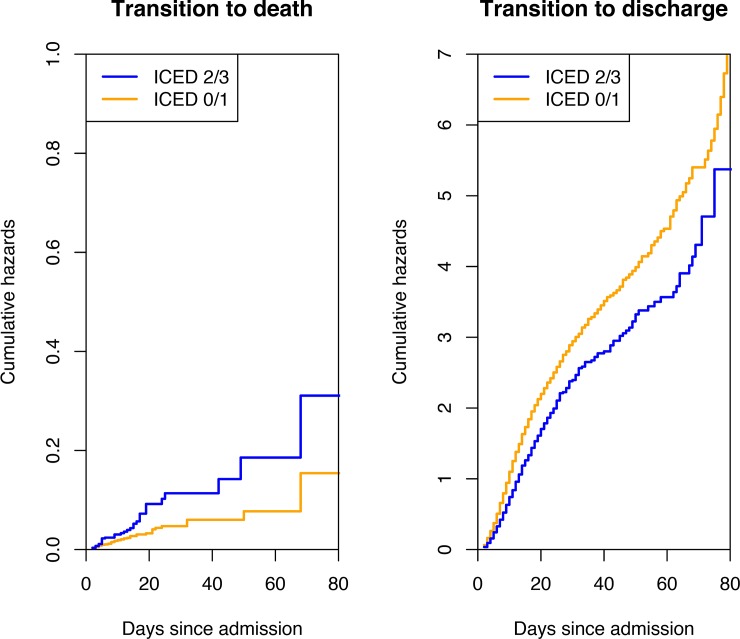
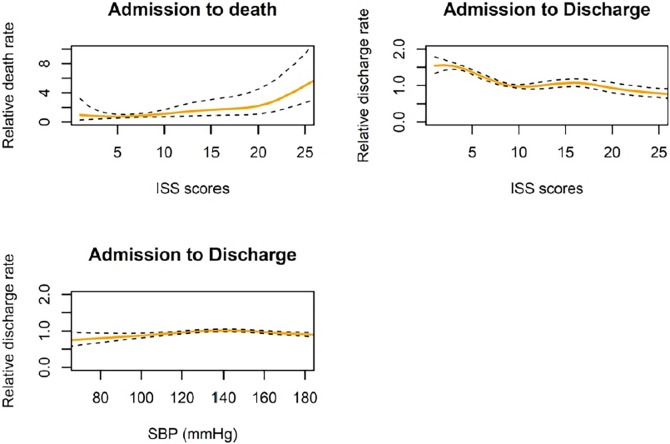
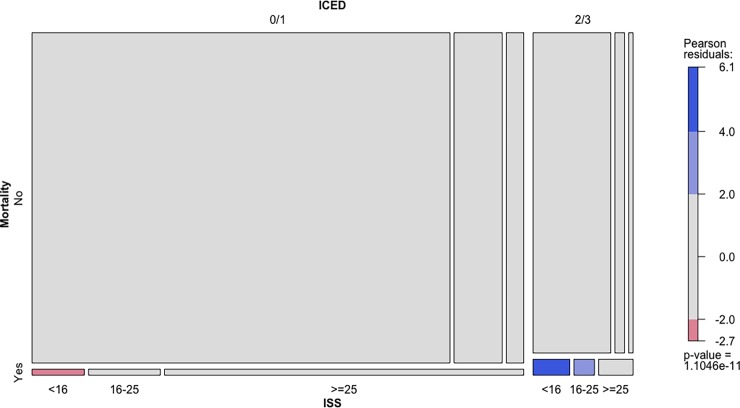
Here we conducted a retrospective analysis of hospital-based trauma registry database for evaluating the impacts of comorbidities on the prognosis for traumatized patients using Index of Coexistent Comorbidity Disease (ICED) scores. We analyzed the data of patients with blunt trauma who visited emergency department between January 1, 2011, and December 31, 2015 in Chang-Gung Memorial Hospital, Keelung branch, a single level I trauma center in the Northern Taiwan. All consecutive patients with blunt trauma who admitted to the intensive care unit or ordinary ward after initial managements in the emergency department were included. We measured the hospital mortality of blunt traumatized patients using alive discharge as a competing risk. To investigate conditional independence of mortality and ICED scores given Injury Severity Score (ISS), we used log-linear models for modeling independence structures. Overall, we included 4997 patients (median age [IQR], 59 years old (44-75 years); 55.3% male). The mortality rate of blunt traumatized patients was higher in the higher ICED scores group compared to lower ICED scores group (4.7% vs 1.8%, p < 0.001). Meanwhile, the higher ICED scores group were associated with older age, higher ISS, and longer hospital stay than lower ICED scores group. Higher ICED group had higher probability of transition-to-death and lower probability of transition-to-discharge under the competing risk model. In the multivariable analysis of transition-specific Cox models, higher ICED group were associated with higher risk for hospital mortality compared to lower ICED group (HR 1.60; [95% CI 1.04-2.47]; p = 0.032). Also, higher ICED group were associated with lower probability of transition-to-discharge (HR 0.79; [95%CI 0.73-0.86]; p < 0.001). Additionally, higher ICED scores accounted for hospital mortality among patients with ISS < 25. In conclusion, our study suggested that severity of comorbidity was associated with higher hospital mortality among traumatized patients, particularly lower ISS.
Conflict of interest statement
Figures
Similar articles
-
Trauma in the elderly: intensive care unit resource use and outcome.J Trauma. 2002 Sep;53(3):407-14. doi: 10.1097/00005373-200209000-00001. J Trauma. 2002. PMID: 12352472
-
Comorbidity-Polypharmacy Score as Predictor of Outcomes in Older Trauma Patients: A Retrospective Validation Study.World J Surg. 2015 Aug;39(8):2068-75. doi: 10.1007/s00268-015-3041-5. World J Surg. 2015. PMID: 25809063
-
Same Abbreviated Injury Scale Values May Be Associated with Different Risks to Mortality in Trauma Patients: A Cross-Sectional Retrospective Study Based on the Trauma Registry System in a Level I Trauma Center.Int J Environ Res Public Health. 2017 Dec 11;14(12):1552. doi: 10.3390/ijerph14121552. Int J Environ Res Public Health. 2017. PMID: 29232883 Free PMC article.
-
Male gender is associated with increased risk for postinjury pneumonia.Shock. 2004 May;21(5):410-4. doi: 10.1097/00024382-200405000-00003. Shock. 2004. PMID: 15087816 Review.
-
Total care of trauma patients from triage to discharge at Chang Gung Memorial Hospital: introducing the development of an iconic acute care surgery system in Taiwan.World J Emerg Surg. 2025 Apr 2;20(1):27. doi: 10.1186/s13017-025-00603-9. World J Emerg Surg. 2025. PMID: 40176141 Free PMC article. Review.
Cited by
-
Opportunities to Improve Palliative Care Delivery in Trauma Critical Illness.Am J Hosp Palliat Care. 2022 Jun;39(6):633-640. doi: 10.1177/10499091211042303. Epub 2021 Sep 1. Am J Hosp Palliat Care. 2022. PMID: 34467775 Free PMC article.
-
Using Partnerships and Multiple Data Sources to Surveil Agricultural Injuries: Considerations and Recommendations.J Agromedicine. 2024 Apr;29(2):197-205. doi: 10.1080/1059924X.2023.2293835. Epub 2023 Dec 18. J Agromedicine. 2024. PMID: 38108301 Free PMC article.
-
Geriatric Trauma - A Rising Tide. Assessing Patient Safety Challenges in a Vulnerable Population Using Norwegian Trauma Registry Data and Focus Group Interviews: Protocol for a Mixed Methods Study.JMIR Res Protoc. 2020 Apr 30;9(4):e15722. doi: 10.2196/15722. JMIR Res Protoc. 2020. PMID: 32352386 Free PMC article.
-
Major trauma and comorbidity: a scoping review.Eur J Trauma Emerg Surg. 2025 Mar 12;51(1):133. doi: 10.1007/s00068-025-02805-x. Eur J Trauma Emerg Surg. 2025. PMID: 40074872 Free PMC article.
-
The role of the American Society of anesthesiologists physical status classification in predicting trauma mortality and outcomes.Am J Surg. 2019 Dec;218(6):1143-1151. doi: 10.1016/j.amjsurg.2019.09.019. Epub 2019 Sep 24. Am J Surg. 2019. PMID: 31575418 Free PMC article.
References
-
- Organization. WH. Global Burden of Disease. http://www.who.int/healthinfo/global_burden_disease/en/ accessed 28 February 2018
-
- Ministry of Health and Welfare, Taiwan. 2016 Statistics of Causes of Death June,2016. Available from: https://dep.mohw.gov.tw/DOS/lp-3352-113.html accessed 28 February 2018
-
- Kahl JE, Calvo RY, Sise MJ, Sise CB, Thorndike JF, Shackford SR. The changing nature of death on the trauma service. J Trauma Acute Care Surg. 2013;75(2):195–201. Epub 2013/07/05. doi: 10.1097/TA.0b013e3182997865 . - DOI - PubMed
-
- Glance LG, Osler TM, Mukamel DB, Dick AW. Outcomes of adult trauma patients admitted to trauma centers in Pennsylvania, 2000–2009. Arch Surg. 2012;147(8):732–7. Epub 2012/08/23. doi: 10.1001/archsurg.2012.1138 . - DOI - PubMed
-
- Kuhne CA, Ruchholtz S, Kaiser GM, Nast-Kolb D. Mortality in severely injured elderly trauma patients—when does age become a risk factor? World J Surg. 2005;29(11):1476–82. Epub 2005/10/18. doi: 10.1007/s00268-005-7796-y . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
