

Quality of Health Care for Children in Australia, 2012-2013
- PMID: 29558552
- PMCID: PMC5885883
- DOI: 10.1001/jama.2018.0162
Quality of Health Care for Children in Australia, 2012-2013
Abstract
Importance: The quality of routine care for children is rarely assessed, and then usually in single settings or for single clinical conditions.
Objective: To estimate the quality of health care for children in Australia in inpatient and ambulatory health care settings.
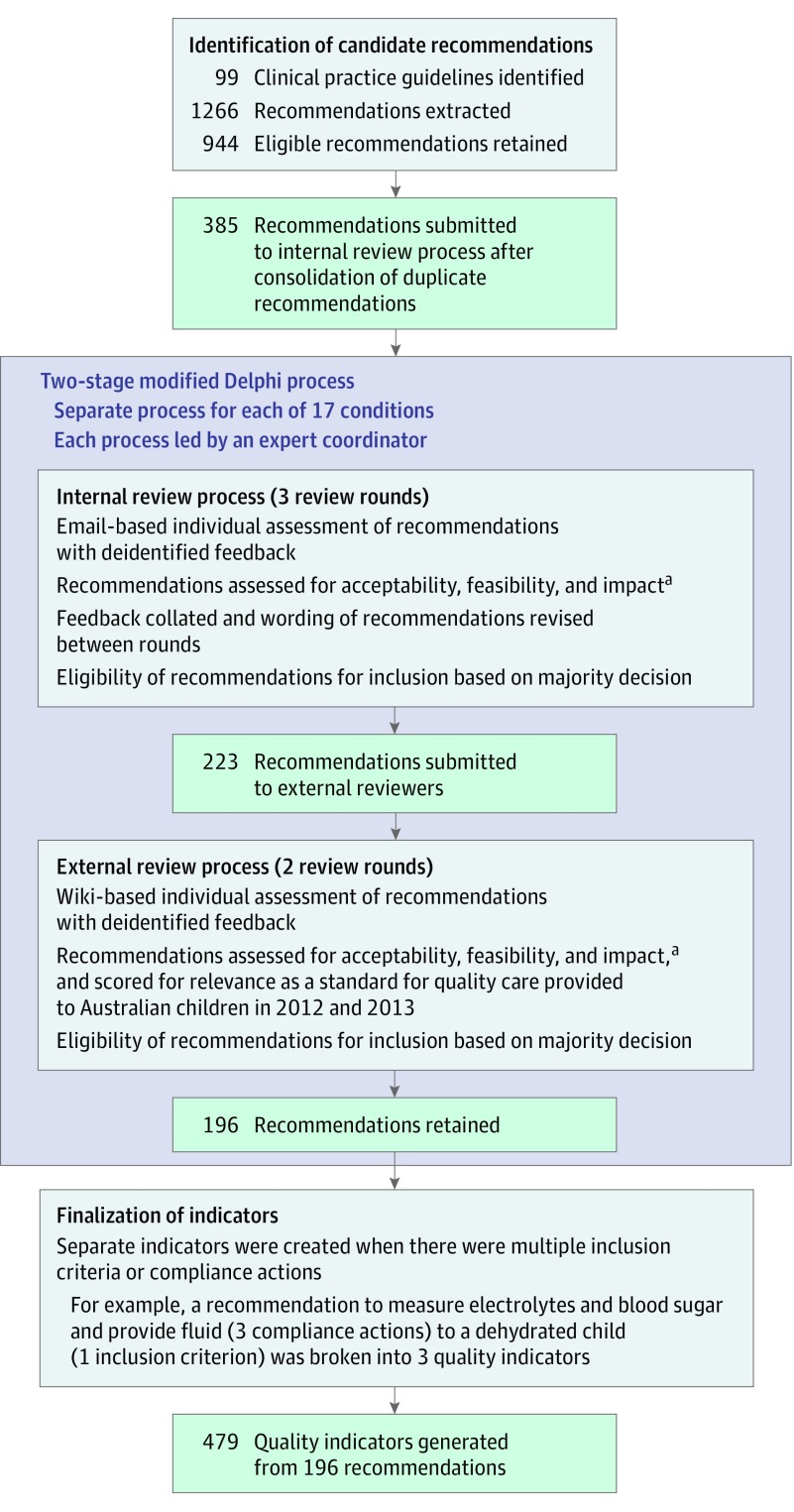
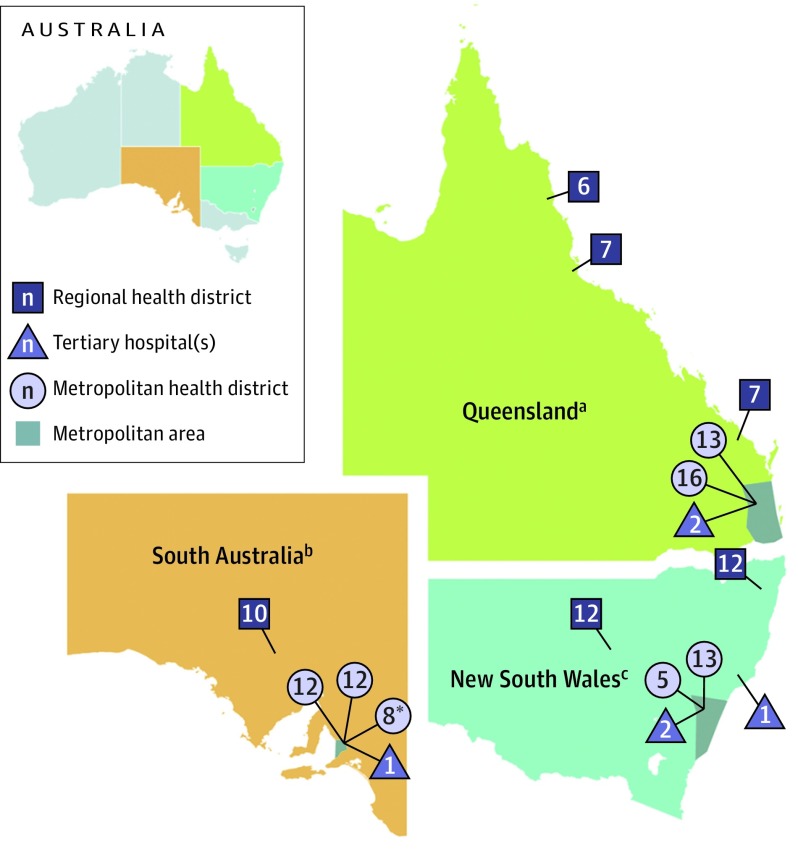
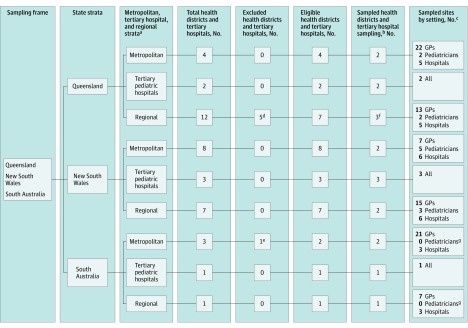
Design, setting, and participants: Multistage stratified sample with medical record review to assess adherence with quality indicators extracted from clinical practice guidelines for 17 common, high-burden clinical conditions (noncommunicable [n = 5], mental health [n = 4], acute infection [n = 7], and injury [n = 1]), such as asthma, attention-deficit/hyperactivity disorder, tonsillitis, and head injury. For these 17 conditions, 479 quality indicators were identified, with the number varying by condition, ranging from 9 for eczema to 54 for head injury. Four hundred medical records were targeted for sampling for each of 15 conditions while 267 records were targeted for anxiety and 133 for depression. Within each selected medical record, all visits for the 17 targeted conditions were identified, and separate quality assessments made for each. Care was evaluated for 6689 children 15 years of age and younger who had 15 240 visits to emergency departments, for inpatient admissions, or to pediatricians and general practitioners in selected urban and rural locations in 3 Australian states. These visits generated 160 202 quality indicator assessments.
Exposures: Quality indicators were identified through a systematic search of local and international guidelines. Individual indicators were extracted from guidelines and assessed using a 2-stage Delphi process.
Main outcomes and measures: Quality of care for each clinical condition and overall.
Results: Of 6689 children with surveyed medical records, 53.6% were aged 0 to 4 years and 55.5% were male. Adherence to quality of care indicators was estimated at 59.8% (95% CI, 57.5%-62.0%; n = 160 202) across the 17 conditions, ranging from a high of 88.8% (95% CI, 83.0%-93.1%; n = 2638) for autism to a low of 43.5% (95% CI, 36.8%-50.4%; n = 2354) for tonsillitis. The mean adherence by condition category was estimated as 60.5% (95% CI, 57.2%-63.8%; n = 41 265) for noncommunicable conditions (range, 52.8%-75.8%); 82.4% (95% CI, 79.0%-85.5%; n = 14 622) for mental health conditions (range, 71.5%-88.8%); 56.3% (95% CI, 53.2%-59.4%; n = 94 037) for acute infections (range, 43.5%-69.8%); and 78.3% (95% CI, 75.1%-81.2%; n = 10 278) for injury.
Conclusions and relevance: Among a sample of children receiving care in Australia in 2012-2013, the overall prevalence of adherence to quality of care indicators for important conditions was not high. For many of these conditions, the quality of care may be inadequate.
Conflict of interest statement
Figures
Comment in
-
Quality of Health Care for Children: The Need for a Firm Foundation of Trustworthy Evidence.JAMA. 2018 Mar 20;319(11):1096-1097. doi: 10.1001/jama.2018.0161. JAMA. 2018. PMID: 29558537 No abstract available.
References
-
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635-2645. - PubMed
-
- Runciman WB, Hunt TD, Hannaford NA, et al. CareTrack: assessing the appropriateness of health care delivery in Australia. Med J Aust. 2012;197(2):100-105. - PubMed
-
- Hathorn C, Alateeqi N, Graham C, O’Hare A. Impact of adherence to best practice guidelines on the diagnostic and assessment services for autism spectrum disorder. J Autism Dev Disord. 2014;44(8):1859-1866. - PubMed
-
- Doherty S, Jones P, Stevens H, Davis L, Ryan N, Treeve V. ‘Evidence-based implementation’ of paediatric asthma guidelines in a rural emergency department. J Paediatr Child Health. 2007;43(9):611-616. - PubMed
-
- Mangione-Smith R, DeCristofaro AH, Setodji CM, et al. The quality of ambulatory care delivered to children in the United States. N Engl J Med. 2007;357(15):1515-1523. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
