

Understanding human genetic factors influencing primaquine safety and efficacy to guide primaquine roll-out in a pre-elimination setting in southern Africa
- PMID: 29558929
- PMCID: PMC5859786
- DOI: 10.1186/s12936-018-2271-z
Understanding human genetic factors influencing primaquine safety and efficacy to guide primaquine roll-out in a pre-elimination setting in southern Africa
Abstract
Background: Primaquine (PQ) is recommended as an addition to standard malaria treatments in pre-elimination settings due to its pronounced activity against mature Plasmodium falciparum gametocytes, the parasite stage responsible for onward transmission to mosquitoes. However, PQ may trigger haemolysis in glucose-6-phosphate dehydrogenase (G6PD)-deficient individuals. Additional human genetic factors, including polymorphisms in the human cytochrome P450 2D6 (CYP2D6) complex, may negatively influence the efficacy of PQ. This study assessed the prevalence of G6PD deficiency and two important CYP2D6 variants in representative pre-elimination settings in South Africa, to inform malaria elimination strategies.
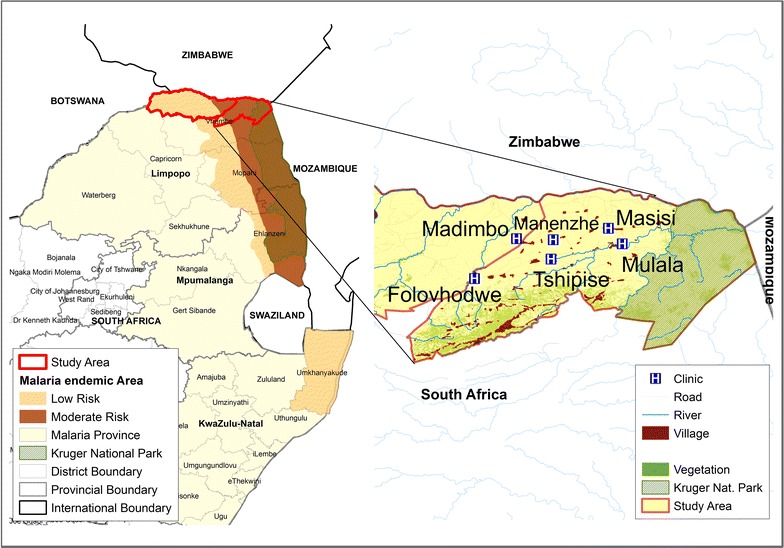
Methods: Volunteers (n = 248) attending six primary health care facilities in a malaria-endemic region of South Africa were enrolled between October and November 2015. G6PD status was determined phenotypically, using a CareStart™ G6PD rapid diagnostic test (RDT), and genotypically for two common African G6PD variants, namely A+ (A376G) and A- (G202A, A542T, G680T & T968C) by PCR, restriction fragment length polymorphisms (RFLP) and DNA sequencing. CYP2D6*4 and CYP2D6*17 variants were determined with PCR and RFLP.
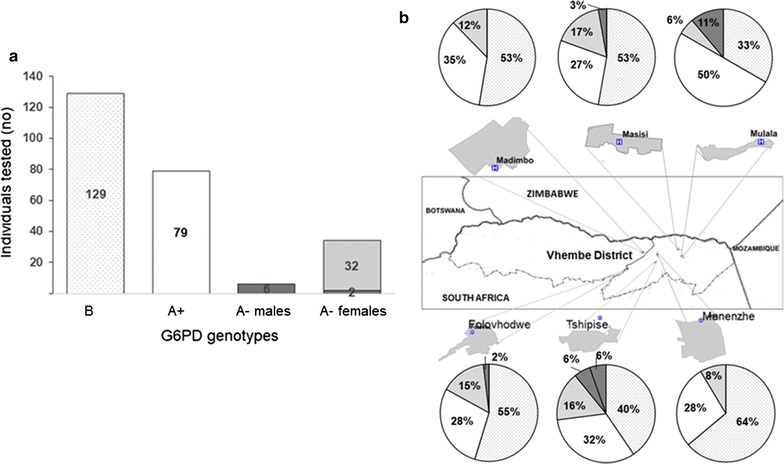
Results: A prevalence of 13% (33/248) G6PD deficiency was observed in the cohort by G6PD RDT whilst by genotypic assessment, 32% (79/248) were A+ and 3.2% were A-, respectively. Among the male participants, 11% (6/55) were G6PD A- hemizygous; among females 1% (2/193) were G6PD A- homozygous and 16% (32/193) G6PD A- heterozygous. The strength of agreement between phenotyping and genotyping result was fair (Cohens Kappa κ = 0.310). The negative predictive value for the G6PD RDT for detecting hemizygous, homozygous and heterozygous individuals was 0.88 (95% CI 0.85-0.91), compared to the more sensitive genotyping. The CYP2D6*4 allele frequencies for CYP2D6*4 (inferred poor metabolizer phenotype) and CYP2D6*17 (inferred intermediate metabolizer phenotype) were 3.2 and 19.5%, respectively.
Conclusions: Phenotypic and genotypic analyses both detected low prevalence of G6PD deficiency and the CYP2D6*4 variants. These findings, combined with increasing data confirming safety of single low-dose PQ in individuals with African variants of G6PD deficiency, supports the deployment of single low-dose PQ as a gametocytocidal drug. PQ would pose minimal risks to the study populations and could be a useful elimination strategy in the study area.
Keywords: CYP2D6; G6PD deficiency; Malaria; Malaria elimination; Primaquine.
Figures
References
-
- World Health Organization . Eliminating malaria. Geneva: World Health Organization; 2016.
-
- World Health Organization . Policy brief on single-dose primaquine as gametocytocide in Plasmodium falciparum malaria. Geneva: World Health Organization; 2015.
-
- Dicko A, Brown JM, Diawara H, Baber I, Mahamar A, Soumare HM, et al. Primaquine to reduce transmission of Plasmodium falciparum malaria in Mali: a single-blind, dose-ranging, adaptive randomised phase 2 trial. Lancet Infect Dis. 2016;16:674–684. doi: 10.1016/S1473-3099(15)00479-X. - DOI - PMC - PubMed
-
- Eziefula AC, Bousema T, Yeung S, Kamya M, Owaraganise A, Gabagaya G, et al. Single dose primaquine for clearance of Plasmodium falciparum gametocytes in children with uncomplicated malaria in Uganda: a randomised, controlled, double-blind, dose-ranging trial. Lancet Infect Dis. 2014;14:130–139. doi: 10.1016/S1473-3099(13)70268-8. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
