

Cerebrospinal fluid in the differential diagnosis of Alzheimer's disease: clinical utility of an extended panel of biomarkers in a specialist cognitive clinic
- PMID: 29558979
- PMCID: PMC5861624
- DOI: 10.1186/s13195-018-0361-3
Cerebrospinal fluid in the differential diagnosis of Alzheimer's disease: clinical utility of an extended panel of biomarkers in a specialist cognitive clinic
Abstract
Background: Cerebrospinal fluid (CSF) biomarkers are increasingly being used to support a diagnosis of Alzheimer's disease (AD). Their clinical utility for differentiating AD from non-AD neurodegenerative dementias, such as dementia with Lewy bodies (DLB) or frontotemporal dementia (FTD), is less well established. We aimed to determine the diagnostic utility of an extended panel of CSF biomarkers to differentiate AD from a range of other neurodegenerative dementias.
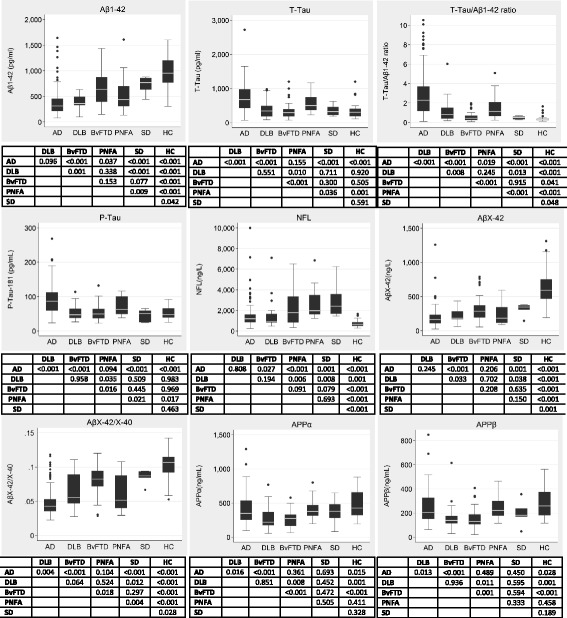
Methods: We used immunoassays to measure conventional CSF markers of amyloid and tau pathology (amyloid beta (Aβ)1-42, total tau (T-tau), and phosphorylated tau (P-tau)) as well as amyloid processing (AβX-38, AβX-40, AβX-42, soluble amyloid precursor protein (sAPP)α, and sAPPβ), large fibre axonal degeneration (neurofilament light chain (NFL)), and neuroinflammation (YKL-40) in 245 patients with a variety of dementias and 30 controls. Patients fulfilled consensus criteria for AD (n = 156), DLB (n = 20), behavioural variant frontotemporal dementia (bvFTD; n = 45), progressive non-fluent aphasia (PNFA; n = 17), and semantic dementia (SD; n = 7); approximately 10% were pathology/genetically confirmed (n = 26). Global tests based on generalised least squares regression were used to determine differences between groups. Non-parametric receiver operating characteristic (ROC) curves and area under the curve (AUC) analyses were used to quantify how well each biomarker discriminated AD from each of the other diagnostic groups (or combinations of groups). CSF cut-points for the major biomarkers found to have diagnostic utility were validated using an independent cohort which included causes of AD (n = 104), DLB (n = 5), bvFTD (n = 12), PNFA (n = 3), SD (n = 9), and controls (n = 10).
Results: There were significant global differences in Aβ1-42, T-tau, T-tau/Aβ1-42 ratio, P-tau-181, NFL, AβX-42, AβX-42/X-40 ratio, APPα, and APPβ between groups. At a fixed sensitivity of 85%, AβX-42/X-40 could differentiate AD from controls, bvFTD, and SD with specificities of 93%, 85%, and 100%, respectively; for T-tau/Aβ1-42 these specificities were 83%, 70%, and 86%. AβX-42/X-40 had similar or higher specificity than Aβ1-42. No biomarker or ratio could differentiate AD from DLB or PNFA with specificity > 50%. Similar sensitivities and specificities were found in the independent validation cohort for differentiating AD and other dementias and in a pathology/genetically confirmed sub-cohort.
Conclusions: CSF AβX-42/X-40 and T-tau/Aβ1-42 ratios have utility in distinguishing AD from controls, bvFTD, and SD. None of the biomarkers tested had good specificity at distinguishing AD from DLB or PNFA.
Keywords: Alzheimer’s disease; Biomarkers; Cerebrospinal fluid; Differential diagnosis.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
The study was conducted in accordance with relevant clinical research regulations, and with ethical approvals in place (Queen Square ethics committee approval reference numbers 13 LO 1155 and 12 LO 1504). Written informed consent was obtained from participants where appropriate.
Consent for publication
Not applicable.
Competing interests
MNR reports consultancy fees from Servier and Merck, paid to the institution outside the submitted work. KB is co-founder of Brain Biomarker Solutions, a GU Holding-based platform company at the University of Gothenburg, and has served on Advisory Boards for IBL International and Roche Diagnostics and given lectures for Fujirebio Europe. NCF reports consultancy fees from Biogen, GSK, Sanofi, Novartis Pharma AG, Eli Lilly, Janssen Alzheimer’s Immunotherapy, and Roche/Genentech paid to the institution. HZ is co-founder of Brain Biomarker Solutions in Gothenburg AB, a GU Venture-based platform company at the University of Gothenburg, Sweden. JMS has received research funding and PET tracer from AVID Radiopharmaceuticals (a wholly owned subsidiary of Eli Lilly), has consulted for Roche, Eli Lilly, Biogen, and Merck, has received royalties from Oxford University Press and Henry Stewart Talks, has given education lectures sponsored by Eli Lilly, and serves on a Data Safety Monitoring Committee for Axon Neuroscience SE outside the submitted work. The remaining authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Olsson B, Lautner R, Andreasson U, Ohrfelt A, Portelius E, Bjerke M, Holtta M, Rosen C, Olsson C, Strobel G, et al. CSF and blood biomarkers for the diagnosis of Alzheimer's disease: a systematic review and meta-analysis. Lancet Neurol. 2016;15:673–684. doi: 10.1016/S1474-4422(16)00070-3. - DOI - PubMed
-
- McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Jr, Kawas CH, Klunk WE, Koroshetz WJ, Manly JJ, Mayeux R, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7:263–269. doi: 10.1016/j.jalz.2011.03.005. - DOI - PMC - PubMed
-
- Wiltfang J, Esselmann H, Bibl M, Hull M, Hampel H, Kessler H, Frolich L, Schroder J, Peters O, Jessen F, et al. Amyloid beta peptide ratio 42/40 but not A beta 42 correlates with phospho-Tau in patients with low- and high-CSF A beta 40 load. J Neurochem. 2007;101:1053–1059. doi: 10.1111/j.1471-4159.2006.04404.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
