

Deep Learning Algorithm for Auto-Delineation of High-Risk Oropharyngeal Clinical Target Volumes With Built-In Dice Similarity Coefficient Parameter Optimization Function
- PMID: 29559291
- PMCID: PMC7473446
- DOI: 10.1016/j.ijrobp.2018.01.114
Deep Learning Algorithm for Auto-Delineation of High-Risk Oropharyngeal Clinical Target Volumes With Built-In Dice Similarity Coefficient Parameter Optimization Function
Abstract
Purpose: Automating and standardizing the contouring of clinical target volumes (CTVs) can reduce interphysician variability, which is one of the largest sources of uncertainty in head and neck radiation therapy. In addition to using uniform margin expansions to auto-delineate high-risk CTVs, very little work has been performed to provide patient- and disease-specific high-risk CTVs. The aim of the present study was to develop a deep neural network for the auto-delineation of high-risk CTVs.
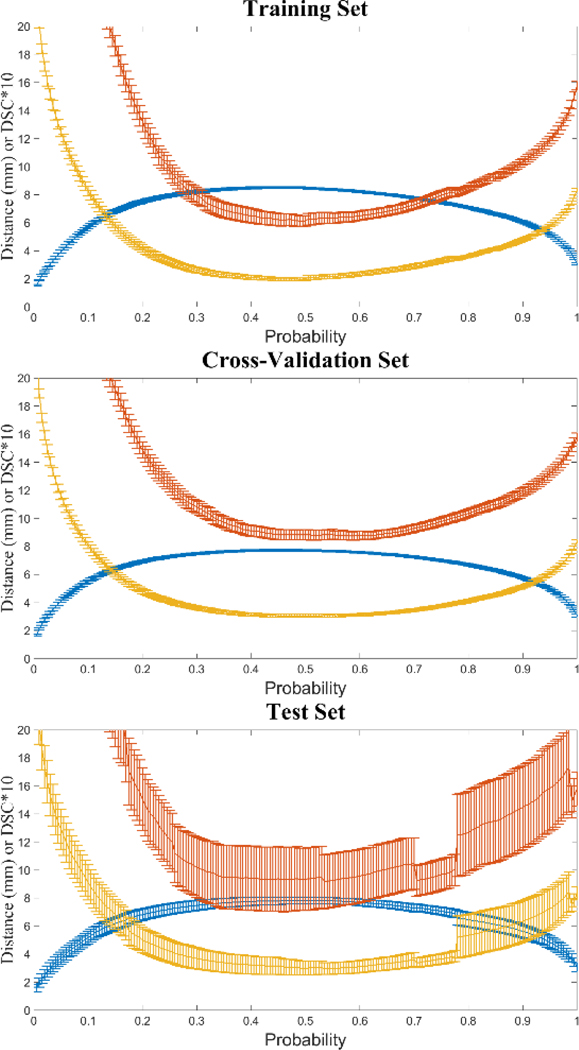
Methods and materials: Fifty-two oropharyngeal cancer patients were selected for the present study. All patients were treated at The University of Texas MD Anderson Cancer Center from January 2006 to August 2010 and had previously contoured gross tumor volumes and CTVs. We developed a deep learning algorithm using deep auto-encoders to identify physician contouring patterns at our institution. These models use distance map information from surrounding anatomic structures and the gross tumor volume as input parameters and conduct voxel-based classification to identify voxels that are part of the high-risk CTV. In addition, we developed a novel probability threshold selection function, based on the Dice similarity coefficient (DSC), to improve the generalization of the predicted volumes. The DSC-based function is implemented during an inner cross-validation loop, and probability thresholds are selected a priori during model parameter optimization. We performed a volumetric comparison between the predicted and manually contoured volumes to assess our model.
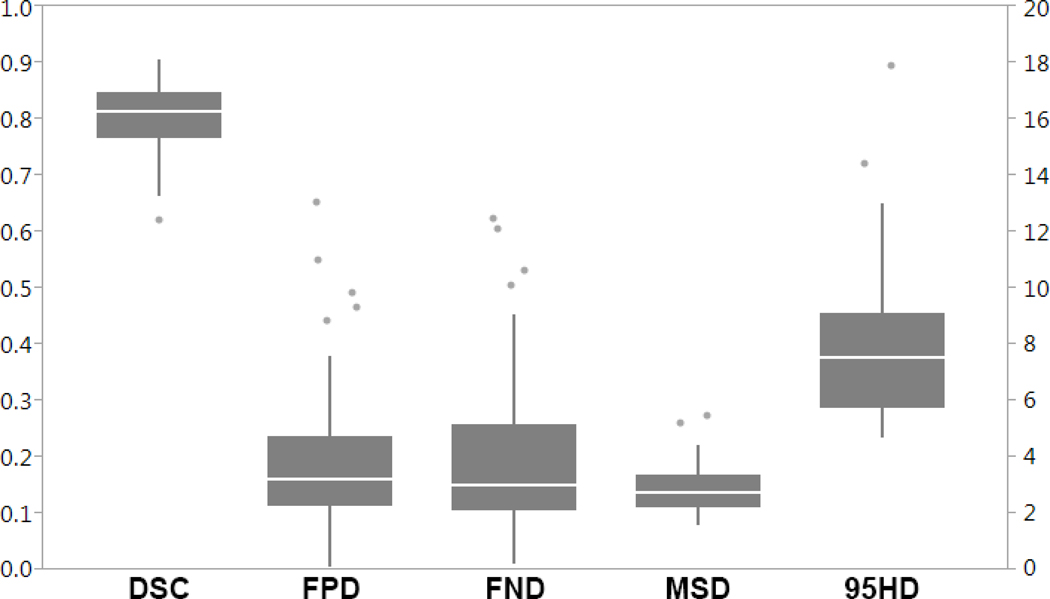
Results: The predicted volumes had a median DSC value of 0.81 (range 0.62-0.90), median mean surface distance of 2.8 mm (range 1.6-5.5), and median 95th Hausdorff distance of 7.5 mm (range 4.7-17.9) when comparing our predicted high-risk CTVs with the physician manual contours.
Conclusions: These predicted high-risk CTVs provided close agreement to the ground-truth compared with current interobserver variability. The predicted contours could be implemented clinically, with only minor or no changes.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest statement: The authors declare no conflicts of interest.
Figures





References
-
- Commission I, Radiation ON. Prescribing, Recording and Reporting Photon Beam Therapy (Supplement to ICRU Report 50). 1999.
-
- Lütgendorf-caucig C, Fotina I, Stock M, Pötter R, Goldner G, Georg D. Feasibility of CBCT-based target and normal structure delineation in prostate cancer radiotherapy : Multi-observer and image multi-modality study. Radiother Oncol. 2011;98:154–161. doi: 10.1016/j.radonc.2010.11.016. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
