

Secondary central nervous system lymphoma: spectrum of morphological MRI appearances
- PMID: 29559780
- PMCID: PMC5856045
- DOI: 10.2147/NDT.S157959
Secondary central nervous system lymphoma: spectrum of morphological MRI appearances
Abstract
Background: Secondary central nervous system lymphoma (SCNSL) is a rare and aggressive disease, which is defined as secondary central nervous system (CNS) involvement in patients with systemic lymphoma. According to previous reports, SCNSL presents mostly with leptomeningeal spread; however, our experience differs. In the present study, we demonstrate the diversity of magnetic resonance imaging (MRI) patterns in SCNSL.
Patients and methods: Initial morphological MRI findings in 21 patients (10 women and 11 men with mean age 62.3±16.2 years) with SCNSL were retrospectively evaluated. All patients suffered from neurological symptoms and underwent MRI, and all cases were histologically verified. Twelve patients were treated by corticosteroids at the time of the initial MRI.
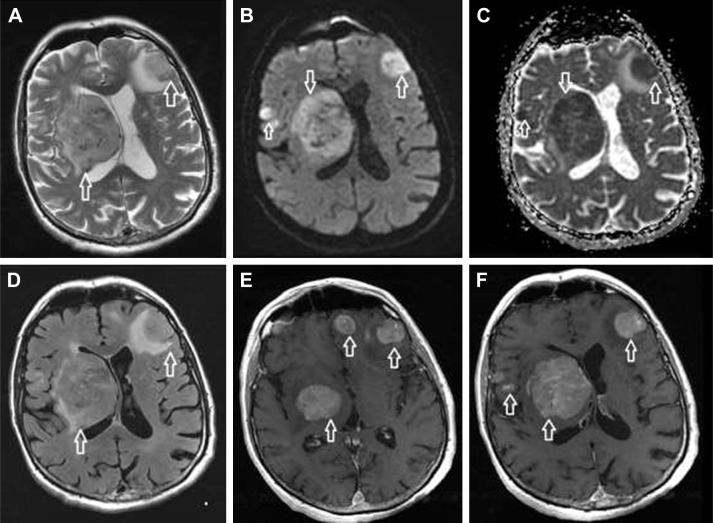
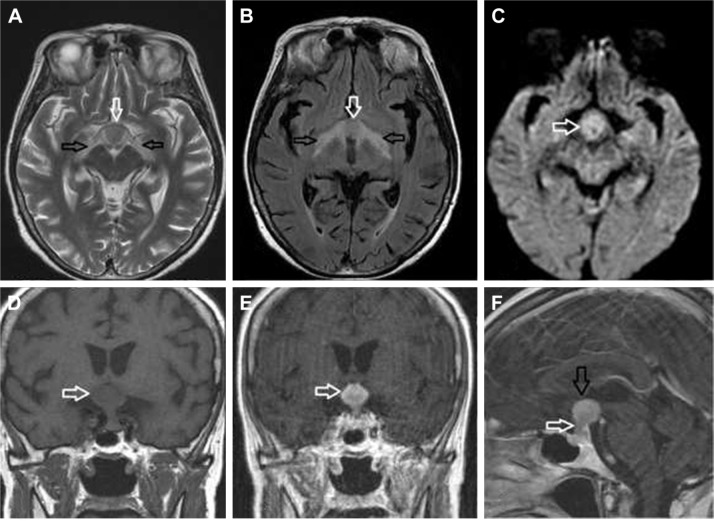
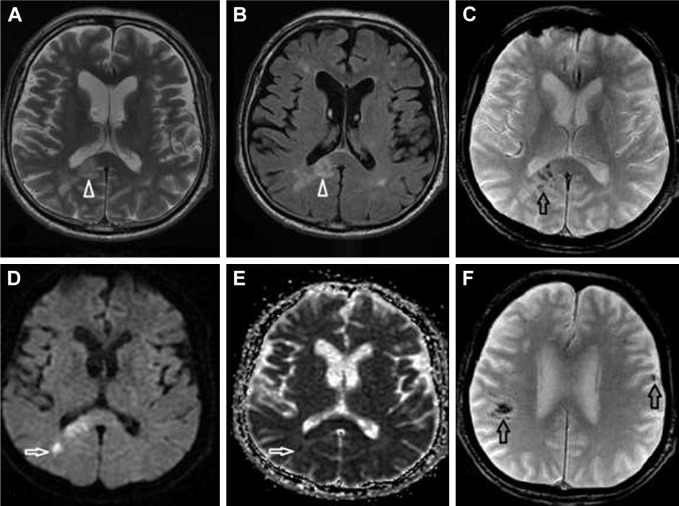
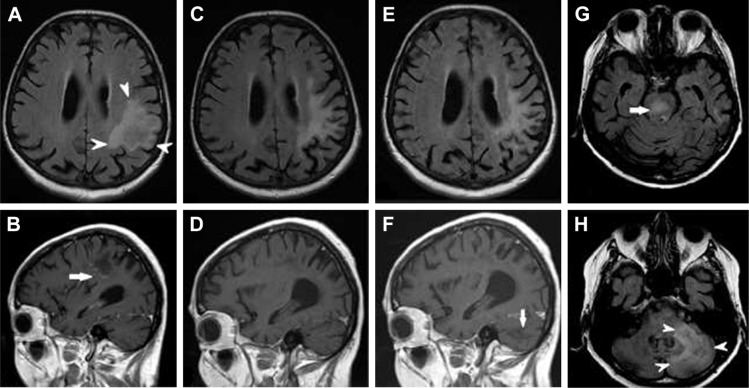
Results: Parenchymal lesions were present in 18 of 21 cases (85.7%), solitary meningeal infiltration was present in 1 patient (4.8%), leptomeningeal infiltration in combination with hypophyseal involvement in 1 patient (4.8%), and solitary involvement of the sixth cranial nerve (CN) was found in 1 patient (4.8%). Multiple lesions were present in 11 of 21 cases (52.4%). Diffusion restriction in all or part of the lesion was detected in 14 of 18 cases (77.8%). All parenchymal lesions had an infiltrative appearance and most enhanced homogenously (11 of 17 cases; 64.7%). A combination of parenchymal and meningeal involvement was found in 10 of 21 cases (47.6%). Infiltration of the CNs, basal ganglia, corpus callosum, and ependyma was present in 8 of 21 cases (38.1%) for each of the abovementioned structures; hypothalamic-hypophyseal axis was affected in 7 of 21 cases (33.3%).
Conclusion: In contrast to previous reports, SCNSL presented as parenchymal disease. MRI is not sufficient for differentiation between primary and secondary CNS lymphoma.
Keywords: brain; magnetic resonance; parenchymal lesions; tumor.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Haioun C, Besson C, Lepage E, et al. Incidence and risk factors of central nervous system relapse in histologically aggressive non-Hodgkin’s lymphoma uniformly treated and receiving intrathecal central nervous system prophylaxis: a GELA study on 974 patients. Groupe d’Etudes des Lymphomes de l’Adulte. Ann Oncol. 2000;11(6):685–690. - PubMed
-
- Jahnke K, Thiel E, Martus P, Schwartz S, Korfel A. Retrospective study of prognostic factors in non-Hodgkin lymphoma secondarily involving the central nervous system. Ann Hematol. 2006;85(1):45–50. - PubMed
-
- Villa D, Connors JM, Shenkier TN, Gascoyne RD, Sehn LH, Savage KJ. Incidence and risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma: the impact of the addition of rituximab to CHOP chemotherapy. Ann Oncol. 2010;21(5):1046–1052. - PubMed
-
- Bierman P, Giglio P. Diagnosis and treatment of central nervous system involvement in non-Hodgkin’s lymphoma. Hematol Oncol Clin North Am. 2005;19(4):597–609. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
